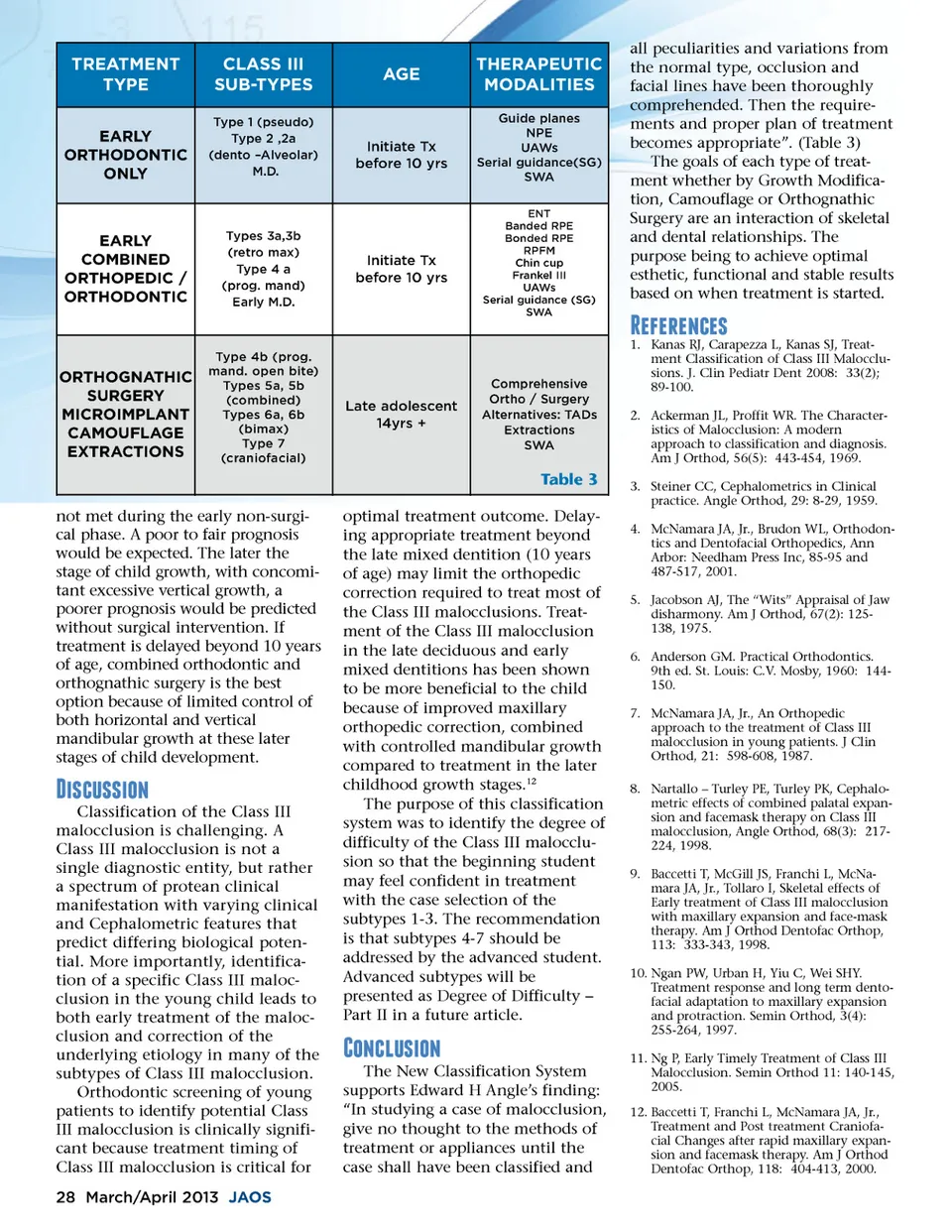
TREATMENT TYPE EARLY ORTHODONTIC ONLY CLASS III SUB-TYPES Type 1 (pseudo) Type 2 ,2a (dento –Alveolar) M.D. AGE THERAPEUTIC MODALITIES Guide planes NPE UAWs Serial guidance(SG) SWA ENT Banded RPE Bonded RPE RPFM Chin cup Frankel III UAWs Serial guidance (SG) SWA Initiate Tx before 10 yrs EARLY COMBINED ORTHOPEDIC / ORTHODONTIC Types 3a,3b (retro max) Type 4 a (prog. mand) Early M.D. Initiate Tx before 10 yrs all peculiarities and variations from the normal type, occlusion and facial lines have been thoroughly comprehended. Then the require-ments and proper plan of treatment becomes appropriate”. (Table 3) The goals of each type of treat-ment whether by Growth Modifica-tion, Camouflage or Orthognathic Surgery are an interaction of skeletal and dental relationships. The purpose being to achieve optimal esthetic, functional and stable results based on when treatment is started. 11)1-'1* ORTHOGNATHIC SURGERY MICROIMPLANT CAMOUFLAGE EXTRACTIONS Type 4b (prog. mand. open bite) Types 5a, 5b (combined) Types 6a, 6b (bimax) Type 7 (craniofacial) Late adolescent 14yrs + Comprehensive Ortho / Surgery Alternatives: TADs Extractions SWA 1. Kanas RJ, Carapezza L, Kanas SJ, Treat-ment Classification of Class III Malocclu-sions. J. Clin Pediatr Dent 2008: 33(2); 89-100. 2. Ackerman JL, Proffit WR. The Character-istics of Malocclusion: A modern approach to classification and diagnosis. Am J Orthod, 56(5): 443-454, 1969. 3. Steiner CC, Cephalometrics in Clinical practice. Angle Orthod, 29: 8-29, 1959. 4. McNamara JA, Jr., Brudon WL, Orthodon-tics and Dentofacial Orthopedics, Ann Arbor: Needham Press Inc, 85-95 and 487-517, 2001. 5. Jacobson AJ, The “Wits” Appraisal of Jaw disharmony. Am J Orthod, 67(2): 125-138, 1975. 6. Anderson GM. Practical Orthodontics. 9th ed. St. Louis: C.V. Mosby, 1960: 144-150. 7. McNamara JA, Jr., An Orthopedic approach to the treatment of Class III malocclusion in young patients. J Clin Orthod, 21: 598-608, 1987. 8. Nartallo – Turley PE, Turley PK, Cephalo-metric effects of combined palatal expan-sion and facemask therapy on Class III malocclusion, Angle Orthod, 68(3): 217-224, 1998. 9. Baccetti T, McGill JS, Franchi L, McNa-mara JA, Jr., Tollaro I, Skeletal effects of Early treatment of Class III malocclusion with maxillary expansion and face-mask therapy. Am J Orthod Dentofac Orthop, 113: 333-343, 1998. 10. Ngan PW, Urban H, Yiu C, Wei SHY. Treatment response and long term dento-facial adaptation to maxillary expansion and protraction. Semin Orthod, 3(4): 255-264, 1997. 11. Ng P, Early Timely Treatment of Class III Malocclusion. Semin Orthod 11: 140-145, 2005. 12. Baccetti T, Franchi L, McNamara JA, Jr., Treatment and Post treatment Craniofa-cial Changes after rapid maxillary expan-sion and facemask therapy. Am J Orthod Dentofac Orthop, 118: 404-413, 2000. Table 3 not met during the early non-surgi-cal phase. A poor to fair prognosis would be expected. The later the stage of child growth, with concomi-tant excessive vertical growth, a poorer prognosis would be predicted without surgical intervention. If treatment is delayed beyond 10 years of age, combined orthodontic and orthognathic surgery is the best option because of limited control of both horizontal and vertical mandibular growth at these later stages of child development. optimal treatment outcome. Delay-ing appropriate treatment beyond the late mixed dentition (10 years of age) may limit the orthopedic correction required to treat most of the Class III malocclusions. Treat-ment of the Class III malocclusion in the late deciduous and early mixed dentitions has been shown to be more beneficial to the child because of improved maxillary orthopedic correction, combined with controlled mandibular growth compared to treatment in the later childhood growth stages. 12 The purpose of this classification system was to identify the degree of difficulty of the Class III malocclu-sion so that the beginning student may feel confident in treatment with the case selection of the subtypes 1-3. The recommendation is that subtypes 4-7 should be addressed by the advanced student. Advanced subtypes will be presented as Degree of Difficulty – Part II in a future article. 0*' **0,-Classification of the Class III malocclusion is challenging. A Class III malocclusion is not a single diagnostic entity, but rather a spectrum of protean clinical manifestation with varying clinical and Cephalometric features that predict differing biological poten-tial. More importantly, identifica-tion of a specific Class III maloc-clusion in the young child leads to both early treatment of the maloc-clusion and correction of the underlying etiology in many of the subtypes of Class III malocclusion. Orthodontic screening of young patients to identify potential Class III malocclusion is clinically signifi-cant because treatment timing of Class III malocclusion is critical for 28 March/April 2013 JAOS e;,-'+ *0,-The New Classification System supports Edward H Angle’s finding: “In studying a case of malocclusion, give no thought to the methods of treatment or appliances until the case shall have been classified and
Journal of the American Orthodontic Society March-April 2013: Page 28