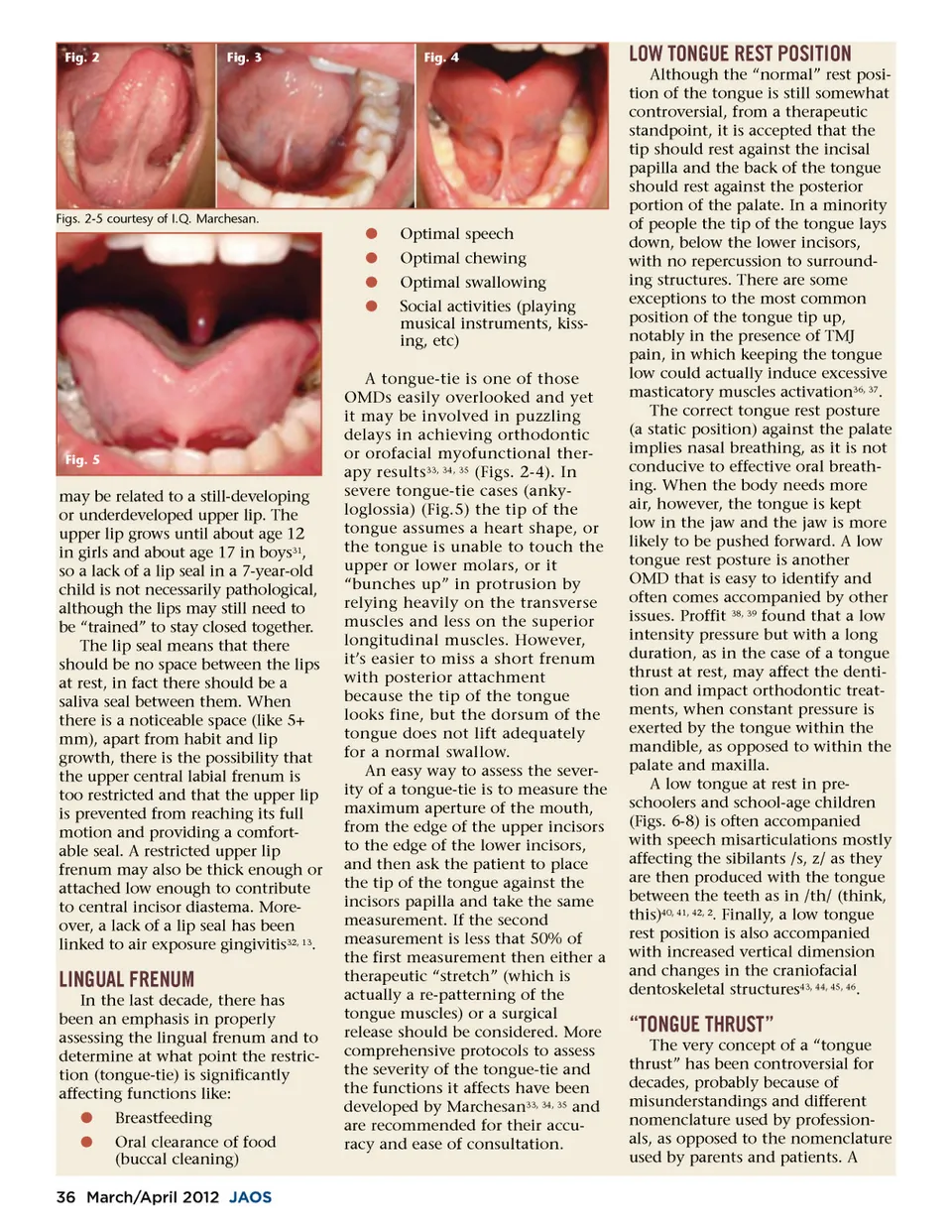
Fig. 2 Fig. 3 Fig. 4 LOW TONGUE REST POSITION Although the “normal” rest posi-tion of the tongue is still somewhat controversial, from a therapeutic standpoint, it is accepted that the tip should rest against the incisal papilla and the back of the tongue should rest against the posterior portion of the palate. In a minority of people the tip of the tongue lays down, below the lower incisors, with no repercussion to surround-ing structures. There are some exceptions to the most common position of the tongue tip up, notably in the presence of TMJ pain, in which keeping the tongue low could actually induce excessive masticatory muscles activation 36, 37 . The correct tongue rest posture (a static position) against the palate implies nasal breathing, as it is not conducive to effective oral breath-ing. When the body needs more air, however, the tongue is kept low in the jaw and the jaw is more likely to be pushed forward. A low tongue rest posture is another OMD that is easy to identify and often comes accompanied by other issues. Proffit 38, 39 found that a low intensity pressure but with a long duration, as in the case of a tongue thrust at rest, may affect the denti-tion and impact orthodontic treat-ments, when constant pressure is exerted by the tongue within the mandible, as opposed to within the palate and maxilla. A low tongue at rest in pre-schoolers and school-age children (Figs. 6-8) is often accompanied with speech misarticulations mostly affecting the sibilants /s, z/ as they are then produced with the tongue between the teeth as in /th/ (think, this) 40, 41, 42, 2 . Finally, a low tongue rest position is also accompanied with increased vertical dimension and changes in the craniofacial dentoskeletal structures 43, 44, 45, 46 . Figs. 2-5 courtesy of I.Q. Marchesan. b b b b Optimal speech Optimal chewing Optimal swallowing Social activities (playing musical instruments, kiss-ing, etc) Fig. 5 may be related to a still-developing or underdeveloped upper lip. The upper lip grows until about age 12 in girls and about age 17 in boys 31 , so a lack of a lip seal in a 7-year-old child is not necessarily pathological, although the lips may still need to be “trained” to stay closed together. The lip seal means that there should be no space between the lips at rest, in fact there should be a saliva seal between them. When there is a noticeable space (like 5+ mm), apart from habit and lip growth, there is the possibility that the upper central labial frenum is too restricted and that the upper lip is prevented from reaching its full motion and providing a comfort-able seal. A restricted upper lip frenum may also be thick enough or attached low enough to contribute to central incisor diastema. More-over, a lack of a lip seal has been linked to air exposure gingivitis 32, 13 . LINGUAL FRENUM In the last decade, there has been an emphasis in properly assessing the lingual frenum and to determine at what point the restric-tion (tongue-tie) is significantly affecting functions like: b b Breastfeeding Oral clearance of food (buccal cleaning) A tongue-tie is one of those OMDs easily overlooked and yet it may be involved in puzzling delays in achieving orthodontic or orofacial myofunctional ther-apy results 33, 34, 35 (Figs. 2-4). In severe tongue-tie cases (anky-loglossia) (Fig.5) the tip of the tongue assumes a heart shape, or the tongue is unable to touch the upper or lower molars, or it “bunches up” in protrusion by relying heavily on the transverse muscles and less on the superior longitudinal muscles. However, it’s easier to miss a short frenum with posterior attachment because the tip of the tongue looks fine, but the dorsum of the tongue does not lift adequately for a normal swallow. An easy way to assess the sever-ity of a tongue-tie is to measure the maximum aperture of the mouth, from the edge of the upper incisors to the edge of the lower incisors, and then ask the patient to place the tip of the tongue against the incisors papilla and take the same measurement. If the second measurement is less that 50% of the first measurement then either a therapeutic “stretch” (which is actually a re-patterning of the tongue muscles) or a surgical release should be considered. More comprehensive protocols to assess the severity of the tongue-tie and the functions it affects have been developed by Marchesan 33, 34, 35 and are recommended for their accu-racy and ease of consultation. “TONGUE THRUST” The very concept of a “tongue thrust” has been controversial for decades, probably because of misunderstandings and different nomenclature used by profession-als, as opposed to the nomenclature used by parents and patients. A 36 March/April 2012 JAOS
Journal of the American Orthodontic Society March-April 2012: Page 36