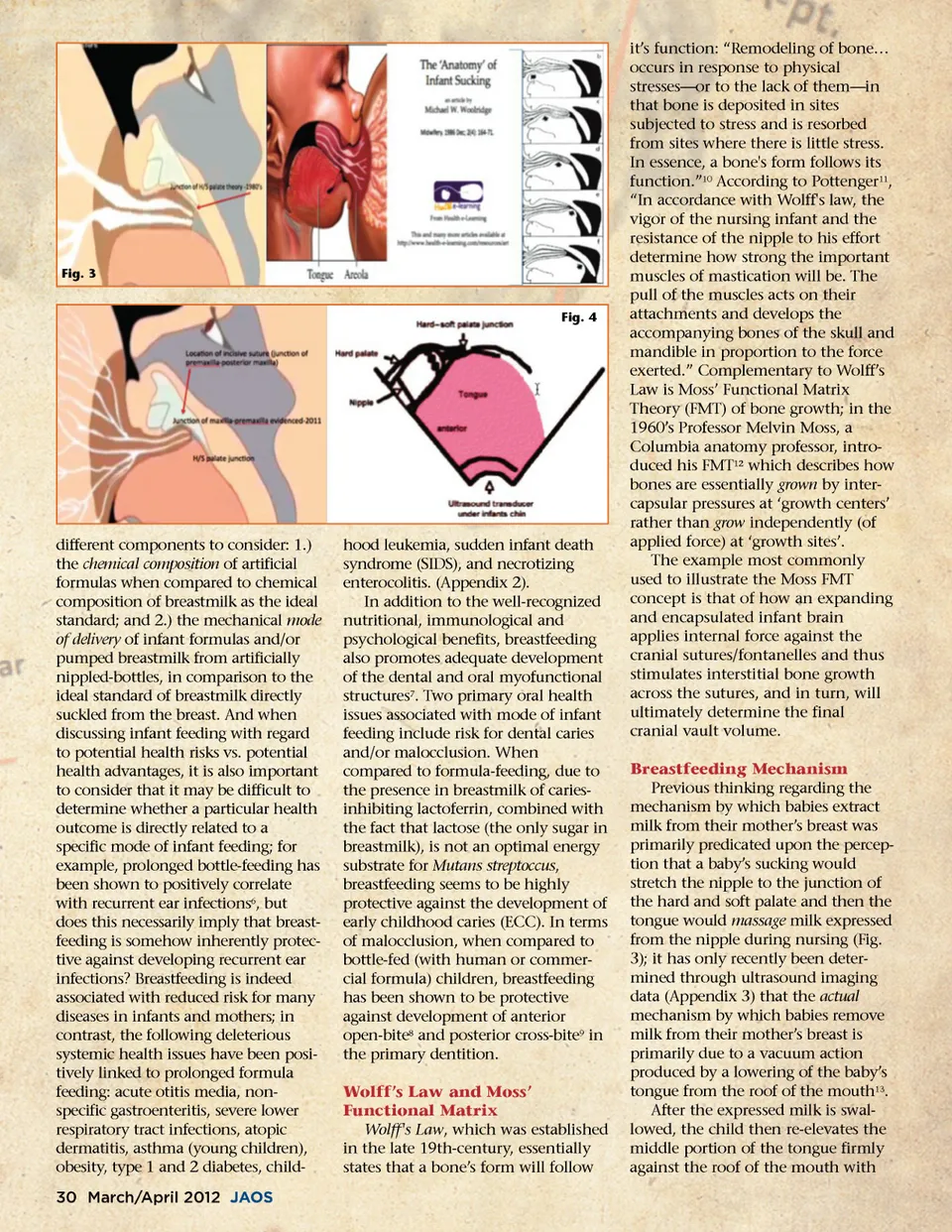
Fig. 3 Fig. 4 different components to consider: 1.) the chemical composition of artificial formulas when compared to chemical composition of breastmilk as the ideal standard; and 2.) the mechanical mode of delivery of infant formulas and/or pumped breastmilk from artificially nippled-bottles, in comparison to the ideal standard of breastmilk directly suckled from the breast. And when discussing infant feeding with regard to potential health risks vs. potential health advantages, it is also important to consider that it may be difficult to determine whether a particular health outcome is directly related to a specific mode of infant feeding; for example, prolonged bottle-feeding has been shown to positively correlate with recurrent ear infections 6 , but does this necessarily imply that breast-feeding is somehow inherently protec-tive against developing recurrent ear infections? Breastfeeding is indeed associated with reduced risk for many diseases in infants and mothers; in contrast, the following deleterious systemic health issues have been posi-tively linked to prolonged formula feeding: acute otitis media, non-specific gastroenteritis, severe lower respiratory tract infections, atopic dermatitis, asthma (young children), obesity, type 1 and 2 diabetes, child-30 March/April 2012 JAOS hood leukemia, sudden infant death syndrome (SIDS), and necrotizing enterocolitis. (Appendix 2). In addition to the well-recognized nutritional, immunological and psychological benefits, breastfeeding also promotes adequate development of the dental and oral myofunctional structures 7 . Two primary oral health issues associated with mode of infant feeding include risk for dental caries and/or malocclusion. When compared to formula-feeding, due to the presence in breastmilk of caries-inhibiting lactoferrin, combined with the fact that lactose (the only sugar in breastmilk), is not an optimal energy substrate for Mutans streptoccus , breastfeeding seems to be highly protective against the development of early childhood caries (ECC). In terms of malocclusion, when compared to bottle-fed (with human or commer-cial formula) children, breastfeeding has been shown to be protective against development of anterior open-bite 8 and posterior cross-bite 9 in the primary dentition. Wolff’s Law and Moss’ Functional Matrix Wolff's Law , which was established in the late 19th-century, essentially states that a bone’s form will follow it’s function: “Remodeling of bone… occurs in response to physical stresses—or to the lack of them—in that bone is deposited in sites subjected to stress and is resorbed from sites where there is little stress. In essence, a bone's form follows its function.” 10 According to Pottenger 11 , “In accordance with Wolff's law, the vigor of the nursing infant and the resistance of the nipple to his effort determine how strong the important muscles of mastication will be. The pull of the muscles acts on their attachments and develops the accompanying bones of the skull and mandible in proportion to the force exerted.” Complementary to Wolff’s Law is Moss’ Functional Matrix Theory (FMT) of bone growth; in the 1960’s Professor Melvin Moss, a Columbia anatomy professor, intro-duced his FMT 12 which describes how bones are essentially grown by inter-capsular pressures at ‘growth centers’ rather than grow independently (of applied force) at ‘growth sites’. The example most commonly used to illustrate the Moss FMT concept is that of how an expanding and encapsulated infant brain applies internal force against the cranial sutures/fontanelles and thus stimulates interstitial bone growth across the sutures, and in turn, will ultimately determine the final cranial vault volume. Breastfeeding Mechanism Previous thinking regarding the mechanism by which babies extract milk from their mother’s breast was primarily predicated upon the percep-tion that a baby’s sucking would stretch the nipple to the junction of the hard and soft palate and then the tongue would massage milk expressed from the nipple during nursing (Fig. 3); it has only recently been deter-mined through ultrasound imaging data (Appendix 3) that the actual mechanism by which babies remove milk from their mother’s breast is primarily due to a vacuum action produced by a lowering of the baby’s tongue from the roof of the mouth 13 . After the expressed milk is swal-lowed, the child then re-elevates the middle portion of the tongue firmly against the roof of the mouth with
Journal of the American Orthodontic Society March-April 2012: Page 30