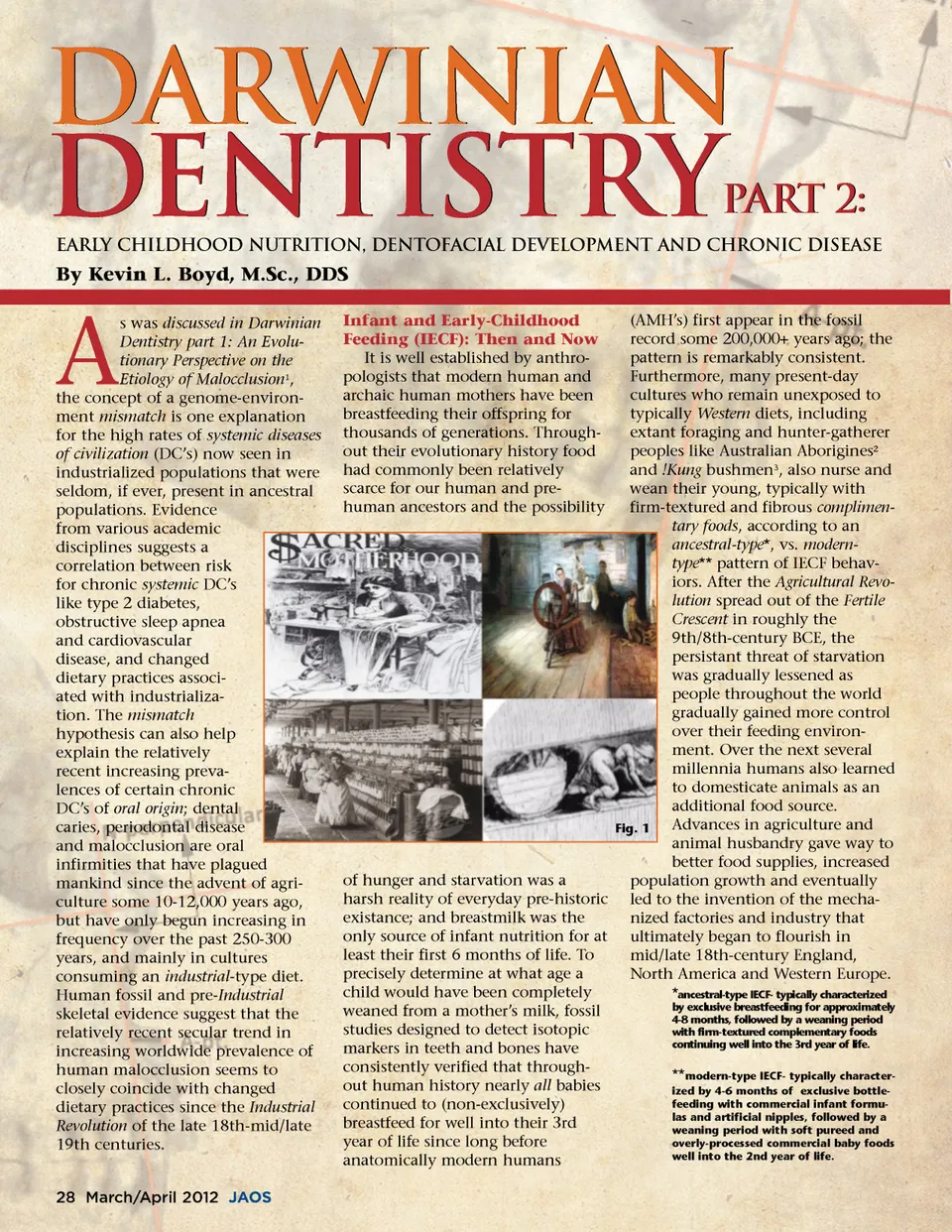
Then: The Long 19th-Century -Women, Infants and Children With the coming of the Industrial Age , many women began to leave their traditional agrarian and cottage industry domestic lifestyles for work in textile mills and as domestic work-ers for middle-and upper-class urban families. The historical era commonly referred to as the Long 19th-Century (1750-1914) 4 is used to describe this period that featured both the emergence of the Industrial Revolution and the consequential Rise of the West . The Long 19th-Century not only brought sweeping changes in agriculture and manufacturing technology, but also ushered in improved transportation and natural resource management that would all eventually, as did the much earlier Agricultural Revolution , spread to the rest of the world. The transition from a manual labor to the new machine-based manufacturing economy seen during this era eventually led to mass migration of human populations from agrarian life to cities; increased income opportunities and general improvements in overall standards of living also contributed to the explo-sive post-Industrial population growth. Affordable and easily accessi-ble highly-processed and calorically-dense foods also contributed to increased standard of living and population density. The traditional roles of women and children were drastically changed by the Long 19th-Century . Prior to the Industrial Revolution , the primary role of children raised in agrarian settings had been as active participants in familial efforts geared towards suste-nance. When urbanized industry became the prevailing way of life, young children were expected to work, usually malnourished, long hours in factories under deplorable conditions. For many European and North American women of the Long 19th-Century , their traditional role in farmhouse and/or domestic cottage industry settings, which was generally conducive to ancestral-type child rear-ing and IECF practices within the home (Fig. 1), was often exchanged for greater income opportunities away from their homes and children. One of the biggest tradeoffs for women who sought better wages away from the home was in having to give up the ability to breastfeed and tradition-ally wean their young beyond the stages of early infancy. Prior to the Industrial Revolution , and usually only during extenuating circumstances like maternal death during childbirth and famine, occasionally newborns had to be fed emergency foods that usually consisted of being wet-nursed and/or fed nutritionally-inferior animal milk and weaned with low-nutrient cereal-based gruels; wet-nursing usually involved the employment of a lactat-ing woman other than the child’s own biological mother. Seemingly superior to other forms of artificial feeding, wet nursing is considered a somewhat inferior substitute as wet nurses did not usually feed children according to an ancestral-type pattern (i.e., ‘on-demand’ and in to the 3rd year of life). As the Industrial Revolution encouraged the employment of women away from their homes and hearths, the newly available highly-processed, calorie-rich and inexpen-sive soft starchy foods were often viewed as a modern miracle . By the middle to end of the 19th-century the trend away from traditional ancestral-type IECF practices was accompanied and gradually replaced by a trend towards feeding babies according to a modern-type IECF regimen that primarily consisted of manufactured animal milk-substitute formulas, newly invented artificial rubber nipples 5 and highly-processed soft-textured gruels. These new commercial baby food products were also often aggressively marketed, not so much as emergency food alternatives for certain babies who couldn’t be traditionally fed according to an ancestral-type IECF regimen, but more often as superior sources of nutrition for all babies; the earliest commercial infant formulas were also marketed as being ideal for individuals of all ages who suffered from chewing disabilities (Fig. 2). Artificial methods of IECF is by no means a recent development in human history. Archaeological sites in the Nile Delta have contained specimens of wooden baby bottles, Fig. 2 and references to artificial feeding are seen in ancient Roman literature and also in the Old Testament. Now: Infant Nutrition… ...Breast is Best? While formula-feeding can be useful and beneficial in terms of convenience and under certain exten-uating circumstances that might preclude breastfeeding, scientific evidence is overwhelming regarding the health advantages of breastmilk in comparison to feeding babies with arti-ficial formulas. According to the World Health Organization (Appendix 1): Breastfeeding is an unequalled way of providing ideal food for the healthy growth and development of infants; it is also an integral part of the reproductive process with important implications for the health of mothers. As a global public health recommendation, infants should be exclusively breastfed for the first six months of life to achieve optimal growth, development and health. There-after, to meet their evolving nutri-tional requirements, infants should receive nutritionally adequate and safe complementary foods while breastfeeding continues for up to two years of age or beyond. Exclu-sive breastfeeding from birth is possible except for a few medical conditions, and unrestricted exclu-sive breastfeeding results in ample milk production. Even though it is a natural act, breastfeeding is also a learned behavior. Virtually all mothers can breastfeed provided they have accurate information, and support within their families and communities and from the health care system. They should also have access to skilled practical help from, for example, trained health workers, lay and peer coun-selors, and certified lactation consultants, who can help to build mothers’ confidence, improve feed-ing technique, and prevent or resolve breastfeeding problems. When discussing issues related to modes of infant feeding and potential health outcomes, it is important to be mindful that there are primarily two www.orthodontics.com March/April 2012 29
Journal of the American Orthodontic Society March-April 2012: Page 29