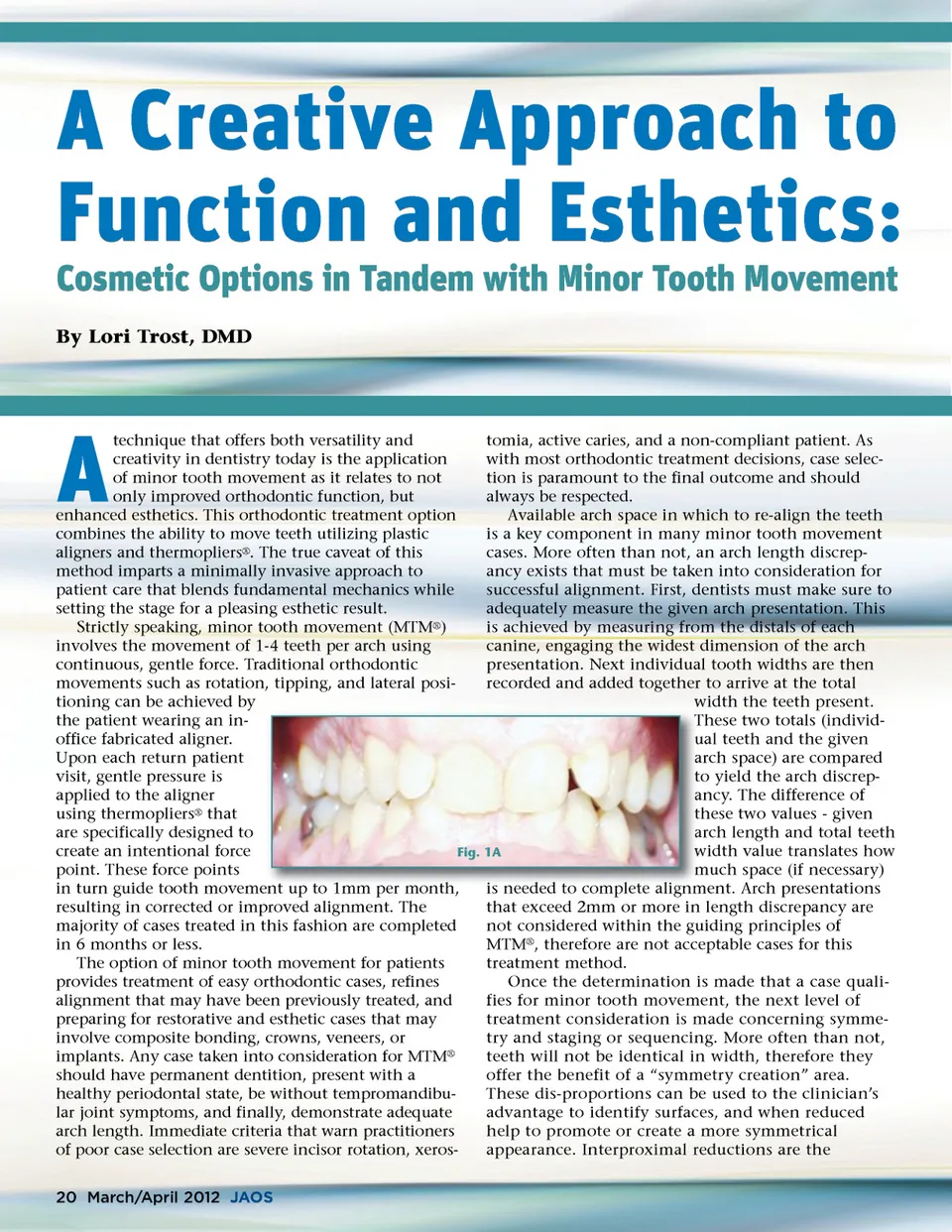
compensation required to align teeth within the current given arch space. If arch space is needed, the clinician has options to procline the teeth -if the opposing arch allows or use interproximal reduction (IPR). Interproximal reduction is the technique used to create interproximal space so that teeth within the arch can pass each other into alignment without colliding. Random tooth reduction is not recom-mended for MTM ® , but rather carefully planned and staged during treatment. The term “enamel contouring” is a much better approach to guarantee not only patient acceptance, but also case success. Done correctly, IPR should not be painful, should always allow adequate remaining tooth structure that is not sensitive, and should respect the initial tooth anatomy to provide pleasing final esthetics. This author recommends performing IPR using a safe-tipped diamond burr, smoothing the affected surfaces with finishing strips, confirming the surfaces with floss for no ledging, and finally measuring newly formed opening with the appropriate interproximal gauge. Critical to minor tooth movement success is model preparation. Teeth that are to be correctly repositioned require two components -force on one side and block-out (the space that the tooth will move into) on the other. This element is central to MTM ® . Block-out material can consist of composite or Triad material. Because these models will undergo a thermoforming or vacuum-forming process -wax should not be used because it will melt and not allow the proper amount of space necessary for correct tooth repositioning. To create the aligner, specific tooth moving plastic is selected with innate properties that remain and stay constant during the fabrication as well as the treatment demands. This author predominately uses either ACE ® or C ® + plastic (Dentsply, Raintree Essix) for all cases. Model preparation consists of spraying the model with a separator, then thermoforming or vacuum-forming the plastic over the model to create the aligner. The aligner is finalized by carefully separating the plastic from the model, trimming and polishing. The final component of minor tooth movement is force. This can be achieved by the use of thermopli-ers ® (Dentsply Raintree Essix) that place directional forces in the plastic aligner on the desired teeth to be moved. Each of the pliers is properly gauged (usually 0.5mm), next heated (according to the plastic selec-tion and its specific thermoplastic properties), and then activated by squeezing a force point into the aligner. Due to the properties of the plastic material, the plastic undergoes a thermal transformation process whereupon when the plier’s force point cools, the plastic will remain in that desired position and not undergo change to create the force point. Rather the thermoplastic properties will retain their newly made position. If heat is not used to warm the ther-moplier, the plastic will subsequently stretch, rebound, or even collapse -thus, the intentional force bump will lessen and not be effective. The brilliance of minor tooth movement truly shines with respect to function, form, and esthetics. Too often Fig. 1B practice, the demand for instant cosmetic in today’s practice gratification dictates treatment offerings and therefore selection/outcome. Dental professionals who learn to understand underlying variations of teeth positions, their inter-occlusal relationships, and enamel etiology benefit greatly from implementing minor tooth move-ment to better their patient’s long term dental presenta-tion. This article will present three cases that demon-strate basic principles of orthodontics as it relates to occlusion to establish improved esthetics, utilizing a minimally invasive approach to patient care. Correction of Deep Overbite Leading to Failed Restorations A fifty-four year old patient presented with good oral hygiene, stable periodontal health, existing restora-tions, and free of caries. However, his chief concern was that his “two front lower teeth fillings were constantly being replaced.” (Fig. 1A) Examination revealed a Class I molar occlusion with maxillary centrals collapsed into a deep overbite arrangement.(Fig. 1B) A standard orthodontic series of photographs were taken. Hybrid polyvinyl impressions were taken of the maxillary and mandibular arches to create both work-ing and study models. Measurements were made from the study model to determine arch length discrepancy and found to be 1.5 mm of needed space. Noteworthy were the disproportionately larger maxillary central teeth as compared to the maxillary lateral teeth as well as the repeatedly broken full surface facial restorations on teeth Nos. 24 and 25. This patient was deemed an excellent candidate for MTM ® treatment, with treat-ment time estimated at 6 months. Treatment Goals Treatment goals for this case were: 1. Tip and rotate maxillary centrals. 2. Focus IPR on distal surfaces of centrals to improve esthetics and golden proportions. 3. Restore teeth Nos. 24 and 25 with composite. 4. Provide proper stabilizing retention. www.orthodontics.com March/April 2012 21
Journal of the American Orthodontic Society March-April 2012: Page 21