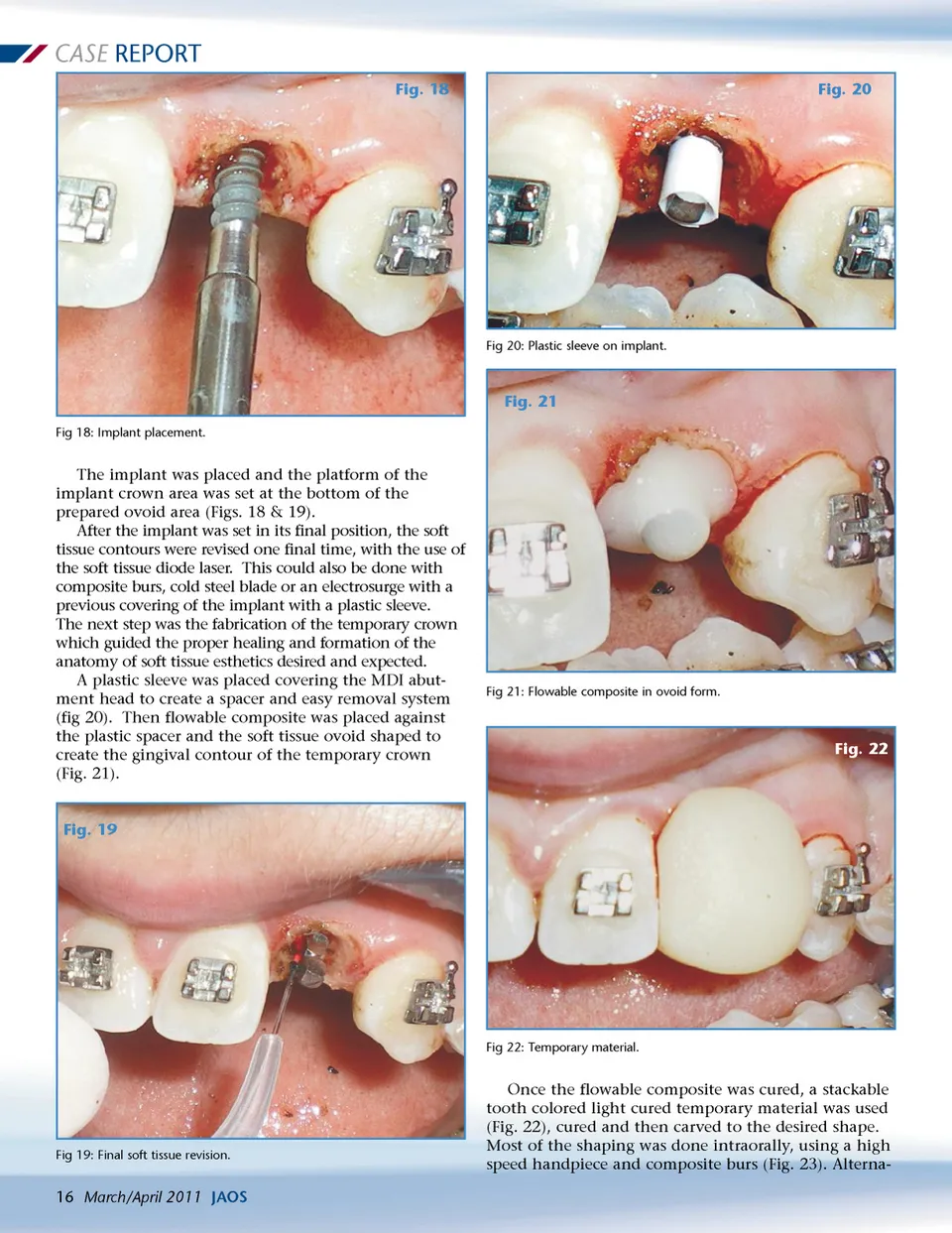
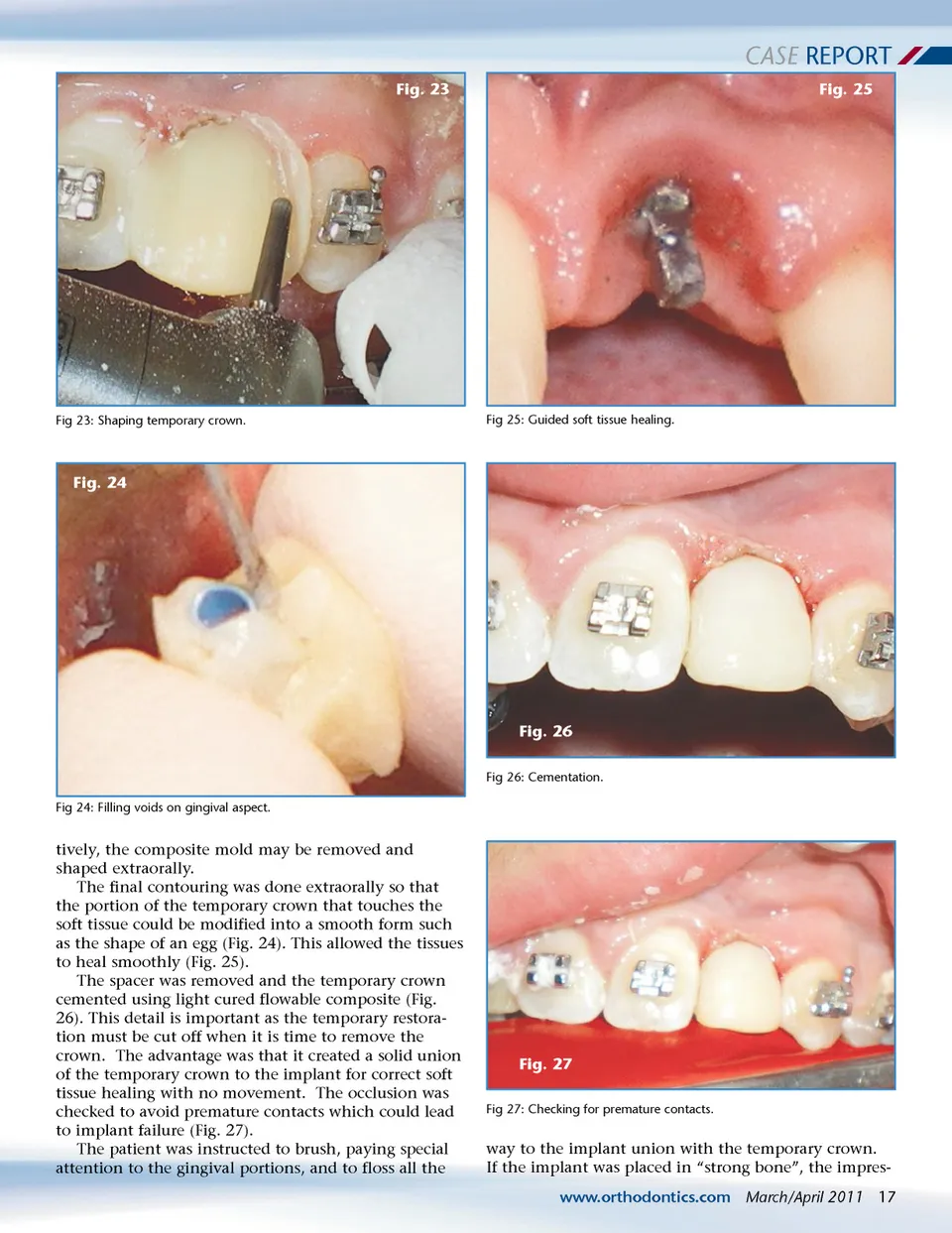
CASE REPORT Fig. 23 Fig. 25 Fig 23: Shaping temporary crown. Fig 25: Guided soft tissue healing. Fig. 24 Fig. 26 Fig 26: Cementation. Fig 24: Filling voids on gingival aspect. tively, the composite mold may be removed and shaped extraorally. The final contouring was done extraorally so that the portion of the temporary crown that touches the soft tissue could be modified into a smooth form such as the shape of an egg (Fig. 24). This allowed the tissues to heal smoothly (Fig. 25). The spacer was removed and the temporary crown cemented using light cured flowable composite (Fig. 26). This detail is important as the temporary restora-tion must be cut off when it is time to remove the crown. The advantage was that it created a solid union of the temporary crown to the implant for correct soft tissue healing with no movement. The occlusion was checked to avoid premature contacts which could lead to implant failure (Fig. 27). The patient was instructed to brush, paying special attention to the gingival portions, and to floss all the Fig. 27 Fig 27: Checking for premature contacts. way to the implant union with the temporary crown. If the implant was placed in “strong bone”, the impres-www.orthodontics.com March/April 2011 17
Journal of the American Orthodontic Society March-April 2011: Page 17