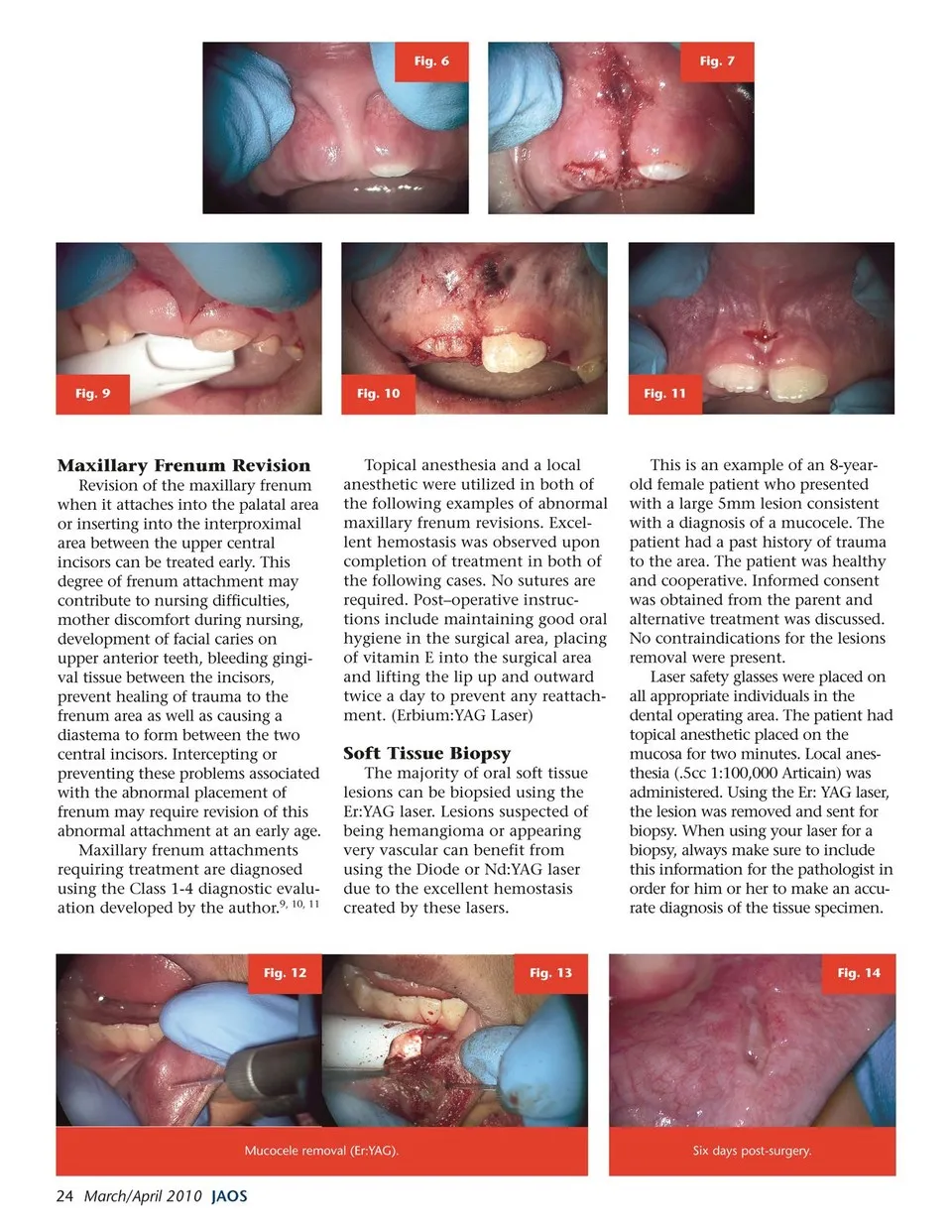
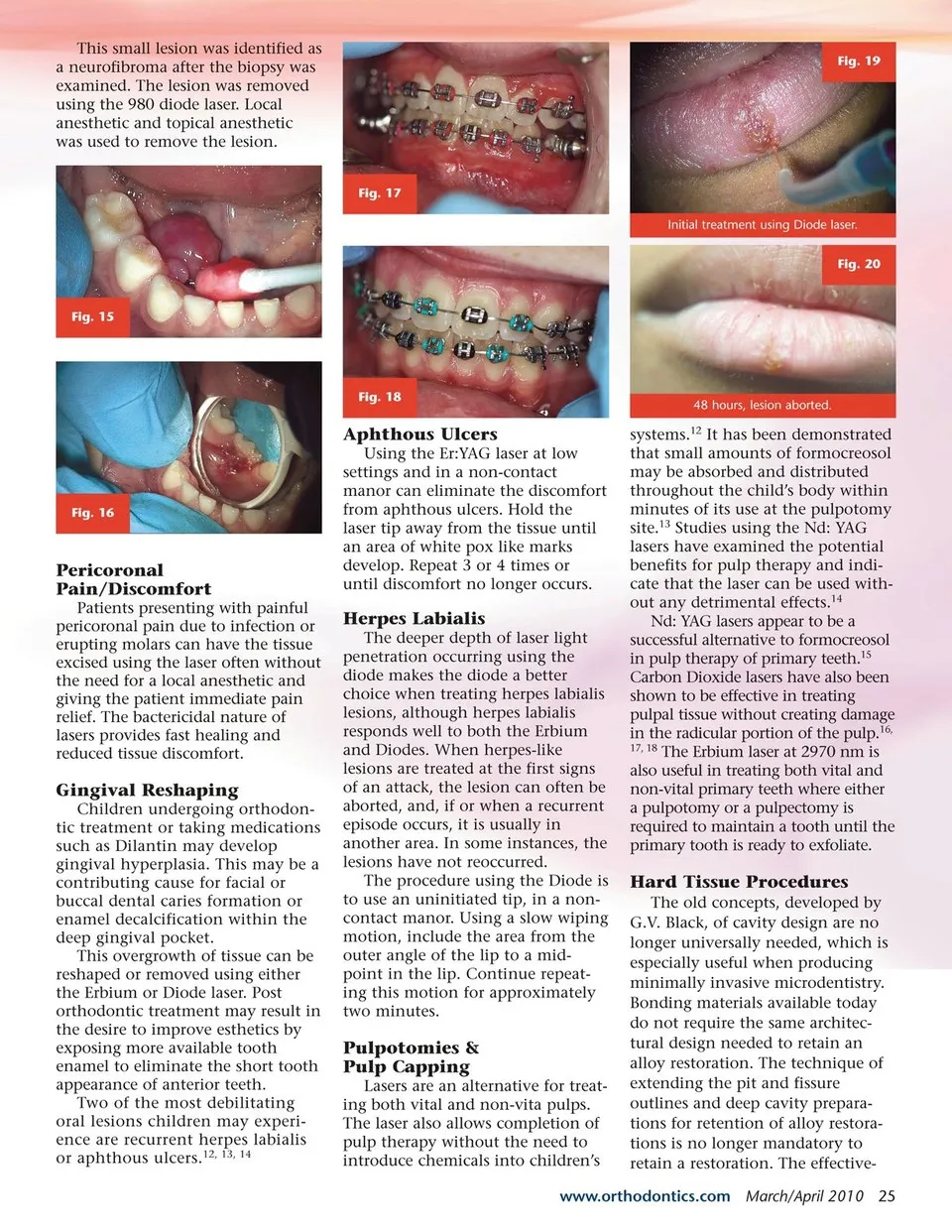
Fig. 6 Fig. 7 Fig. 9 Fig. 10 Fig. 11 Maxillary Frenum Revision Revision of the maxillary frenum when it attaches into the palatal area or inserting into the interproximal area between the upper central incisors can be treated early. This degree of frenum attachment may contribute to nursing difficulties, mother discomfort during nursing, development of facial caries on upper anterior teeth, bleeding gingi- val tissue between the incisors, prevent healing of trauma to the frenum area as well as causing a diastema to form between the two central incisors. Intercepting or preventing these problems associated with the abnormal placement of frenum may require revision of this abnormal attachment at an early age. Maxillary frenum attachments requiring treatment are diagnosed using the Class 1-4 diagnostic evalu- ation developed by the author.9, 10, 11 Fig. 12 Topical anesthesia and a local anesthetic were utilized in both of the following examples of abnormal maxillary frenum revisions. Excel- lent hemostasis was observed upon completion of treatment in both of the following cases. No sutures are required. Post–operative instruc- tions include maintaining good oral hygiene in the surgical area, placing of vitamin E into the surgical area and lifting the lip up and outward twice a day to prevent any reattach- ment. (Erbium:YAG Laser) Soft Tissue Biopsy The majority of oral soft tissue lesions can be biopsied using the Er:YAG laser. Lesions suspected of being hemangioma or appearing very vascular can benefit from using the Diode or Nd:YAG laser due to the excellent hemostasis created by these lasers. Fig. 13 This is an example of an 8-year- old female patient who presented with a large 5mm lesion consistent with a diagnosis of a mucocele. The patient had a past history of trauma to the area. The patient was healthy and cooperative. Informed consent was obtained from the parent and alternative treatment was discussed. No contraindications for the lesions removal were present. Laser safety glasses were placed on all appropriate individuals in the dental operating area. The patient had topical anesthetic placed on the mucosa for two minutes. Local anes- thesia (.5cc 1:100,000 Articain) was administered. Using the Er: YAG laser, the lesion was removed and sent for biopsy. When using your laser for a biopsy, always make sure to include this information for the pathologist in order for him or her to make an accu- rate diagnosis of the tissue specimen. Fig. 14 Mucocele removal (Er:YAG). 24 March/April 2010 JAOS Six days post-surgery.
Journal of the American Orthodontic Society March - April 2010: Page 24