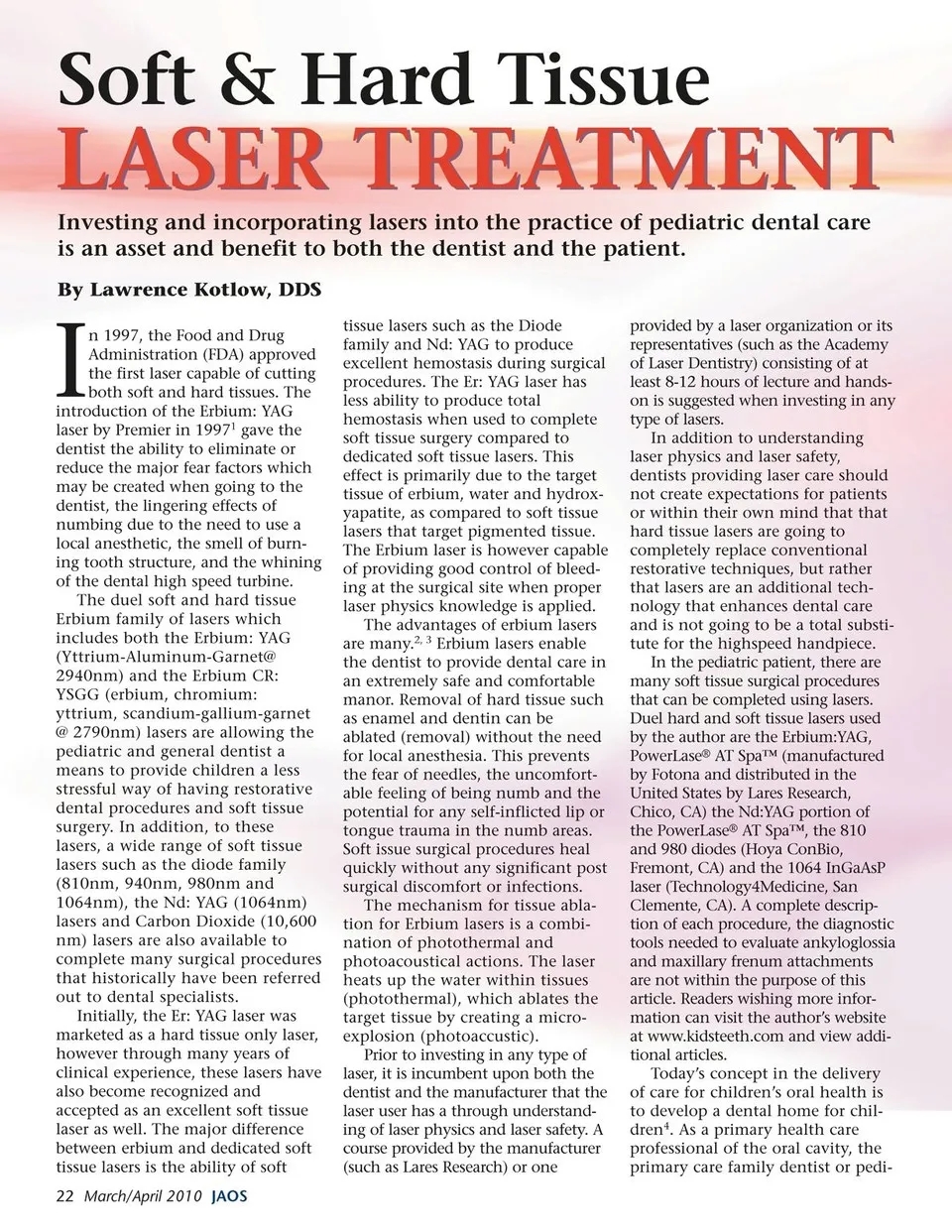
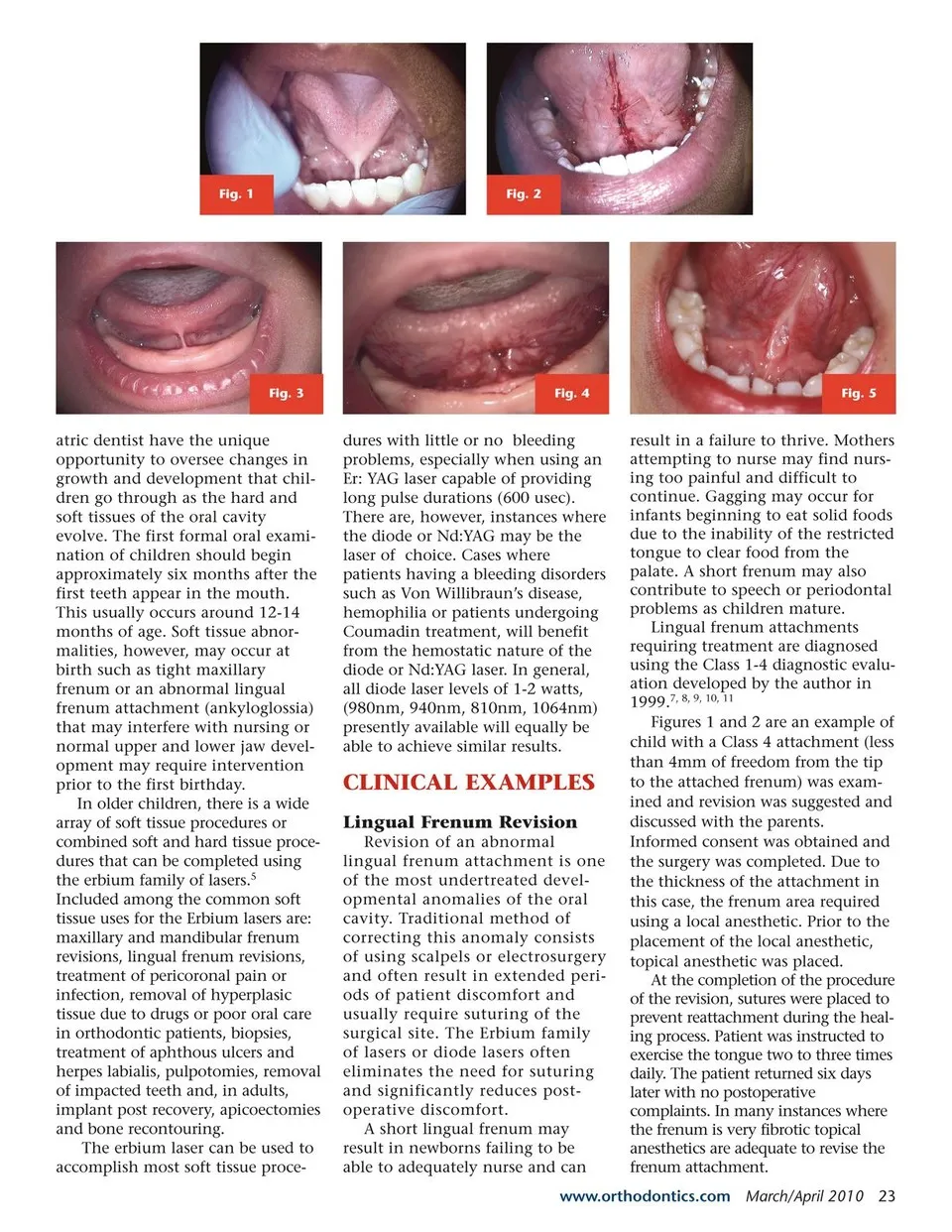
Fig. 1 Fig. 2 Fig. 3 atric dentist have the unique opportunity to oversee changes in growth and development that chil- dren go through as the hard and soft tissues of the oral cavity evolve. The first formal oral exami- nation of children should begin approximately six months after the first teeth appear in the mouth. This usually occurs around 12-14 months of age. Soft tissue abnor- malities, however, may occur at birth such as tight maxillary frenum or an abnormal lingual frenum attachment (ankyloglossia) that may interfere with nursing or normal upper and lower jaw devel- opment may require intervention prior to the first birthday. In older children, there is a wide array of soft tissue procedures or combined soft and hard tissue proce- dures that can be completed using the erbium family of lasers.5 Included among the common soft tissue uses for the Erbium lasers are: maxillary and mandibular frenum revisions, lingual frenum revisions, treatment of pericoronal pain or infection, removal of hyperplasic tissue due to drugs or poor oral care in orthodontic patients, biopsies, treatment of aphthous ulcers and herpes labialis, pulpotomies, removal of impacted teeth and, in adults, implant post recovery, apicoectomies and bone recontouring. The erbium laser can be used to accomplish most soft tissue proce- Fig. 4 dures with little or no bleeding problems, especially when using an Er: YAG laser capable of providing long pulse durations (600 usec). There are, however, instances where the diode or Nd:YAG may be the laser of choice. Cases where patients having a bleeding disorders such as Von Willibraun’s disease, hemophilia or patients undergoing Coumadin treatment, will benefit from the hemostatic nature of the diode or Nd:YAG laser. In general, all diode laser levels of 1-2 watts, (980nm, 940nm, 810nm, 1064nm) presently available will equally be able to achieve similar results. CLINICAL EXAMPLES Lingual Frenum Revision Revision of an abnormal lingual frenum attachment is one of the most undertreated devel- opmental anomalies of the oral cavity. Traditional method of correcting this anomaly consists of using scalpels or electrosurgery and often result in extended peri- ods of patient discomfort and usually require suturing of the surgical site. The Erbium family of lasers or diode lasers often eliminates the need for suturing and significantly reduces post- operative discomfort. A short lingual frenum may result in newborns failing to be able to adequately nurse and can Fig. 5 result in a failure to thrive. Mothers attempting to nurse may find nurs- ing too painful and difficult to continue. Gagging may occur for infants beginning to eat solid foods due to the inability of the restricted tongue to clear food from the palate. A short frenum may also contribute to speech or periodontal problems as children mature. Lingual frenum attachments requiring treatment are diagnosed using the Class 1-4 diagnostic evalu- ation developed by the author in 1999.7, 8, 9, 10, 11 Figures 1 and 2 are an example of child with a Class 4 attachment (less than 4mm of freedom from the tip to the attached frenum) was exam- ined and revision was suggested and discussed with the parents. Informed consent was obtained and the surgery was completed. Due to the thickness of the attachment in this case, the frenum area required using a local anesthetic. Prior to the placement of the local anesthetic, topical anesthetic was placed. At the completion of the procedure of the revision, sutures were placed to prevent reattachment during the heal- ing process. Patient was instructed to exercise the tongue two to three times daily. The patient returned six days later with no postoperative complaints. In many instances where the frenum is very fibrotic topical anesthetics are adequate to revise the frenum attachment. www.orthodontics.com March/April 2010 23
Journal of the American Orthodontic Society March - April 2010: Page 23