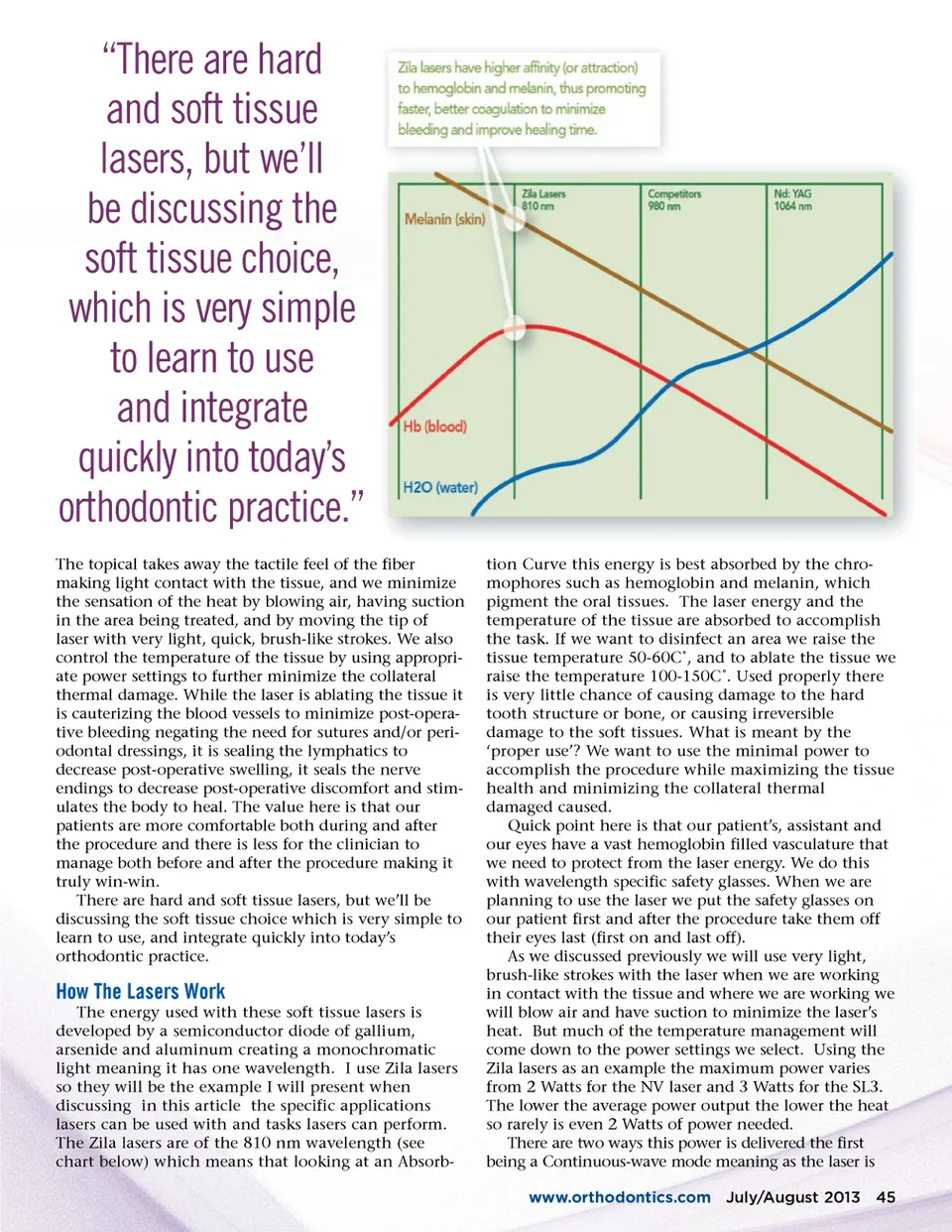
“There are hard and soft tissue lasers, but we’ll be discussing the soft tissue choice, which is very simple to learn to use and integrate quickly into today’s orthodontic practice.” The topical takes away the tactile feel of the fiber making light contact with the tissue, and we minimize the sensation of the heat by blowing air, having suction in the area being treated, and by moving the tip of laser with very light, quick, brush-like strokes. We also control the temperature of the tissue by using appropri-ate power settings to further minimize the collateral thermal damage. While the laser is ablating the tissue it is cauterizing the blood vessels to minimize post-opera-tive bleeding negating the need for sutures and/or peri-odontal dressings, it is sealing the lymphatics to decrease post-operative swelling, it seals the nerve endings to decrease post-operative discomfort and stim-ulates the body to heal. The value here is that our patients are more comfortable both during and after the procedure and there is less for the clinician to manage both before and after the procedure making it truly win-win. There are hard and soft tissue lasers, but we’ll be discussing the soft tissue choice which is very simple to learn to use, and integrate quickly into today’s orthodontic practice. tion Curve this energy is best absorbed by the chro-mophores such as hemoglobin and melanin, which pigment the oral tissues. The laser energy and the temperature of the tissue are absorbed to accomplish the task. If we want to disinfect an area we raise the tissue temperature 50-60C˚, and to ablate the tissue we raise the temperature 100-150C˚. Used properly there is very little chance of causing damage to the hard tooth structure or bone, or causing irreversible damage to the soft tissues. What is meant by the ‘proper use’? We want to use the minimal power to accomplish the procedure while maximizing the tissue health and minimizing the collateral thermal damaged caused. Quick point here is that our patient’s, assistant and our eyes have a vast hemoglobin filled vasculature that we need to protect from the laser energy. We do this with wavelength specific safety glasses. When we are planning to use the laser we put the safety glasses on our patient first and after the procedure take them off their eyes last (first on and last off). As we discussed previously we will use very light, brush-like strokes with the laser when we are working in contact with the tissue and where we are working we will blow air and have suction to minimize the laser’s heat. But much of the temperature management will come down to the power settings we select. Using the Zila lasers as an example the maximum power varies from 2 Watts for the NV laser and 3 Watts for the SL3. The lower the average power output the lower the heat so rarely is even 2 Watts of power needed. There are two ways this power is delivered the first being a Continuous-wave mode meaning as the laser is www.orthodontics.com July/August 2013 45 How The Lasers Work The energy used with these soft tissue lasers is developed by a semiconductor diode of gallium, arsenide and aluminum creating a monochromatic light meaning it has one wavelength. I use Zila lasers so they will be the example I will present when discussing in this article the specific applications lasers can be used with and tasks lasers can perform. The Zila lasers are of the 810 nm wavelength (see chart below) which means that looking at an Absorb-
Journal of the American Orthodontic Society July-August 2013 Buyer's Guide: Page 45