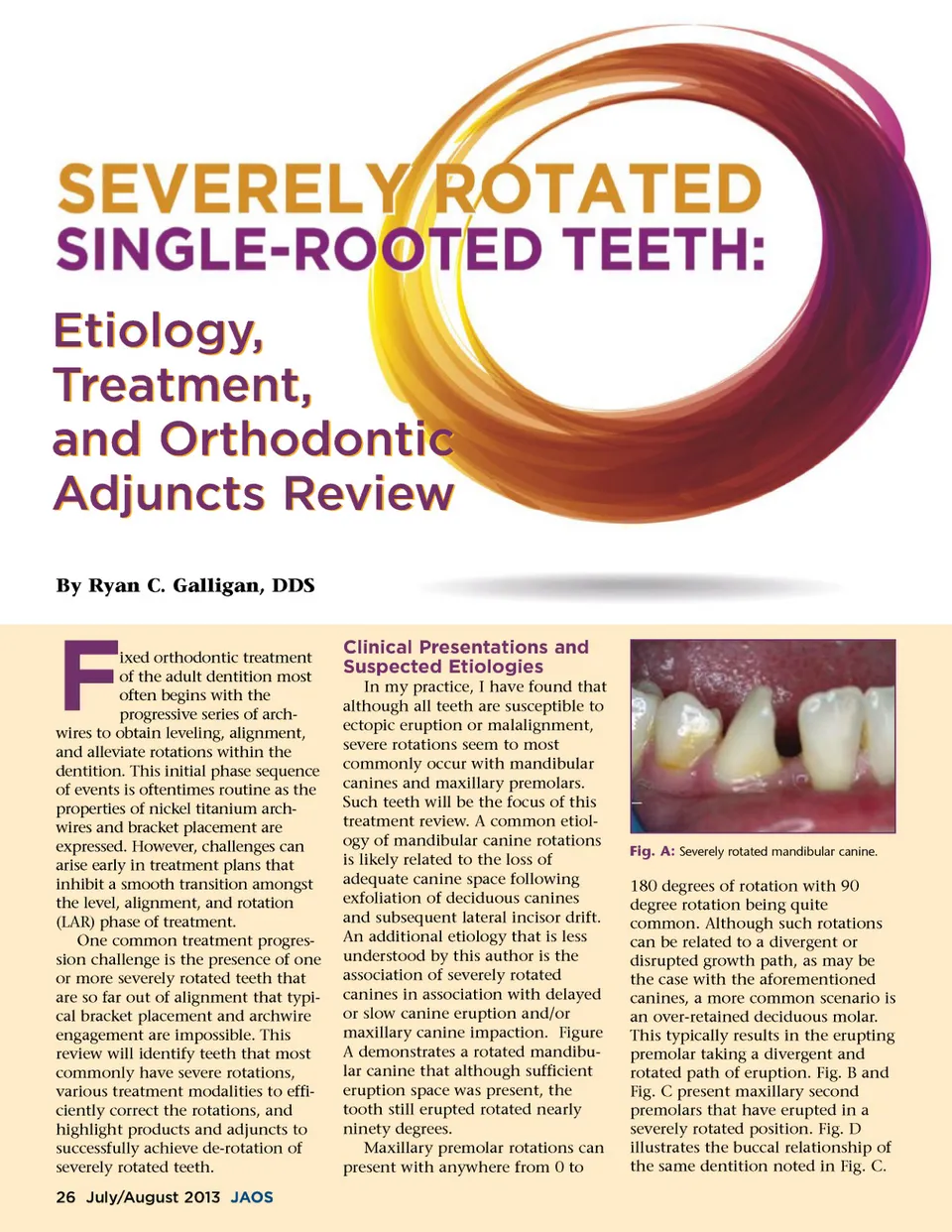
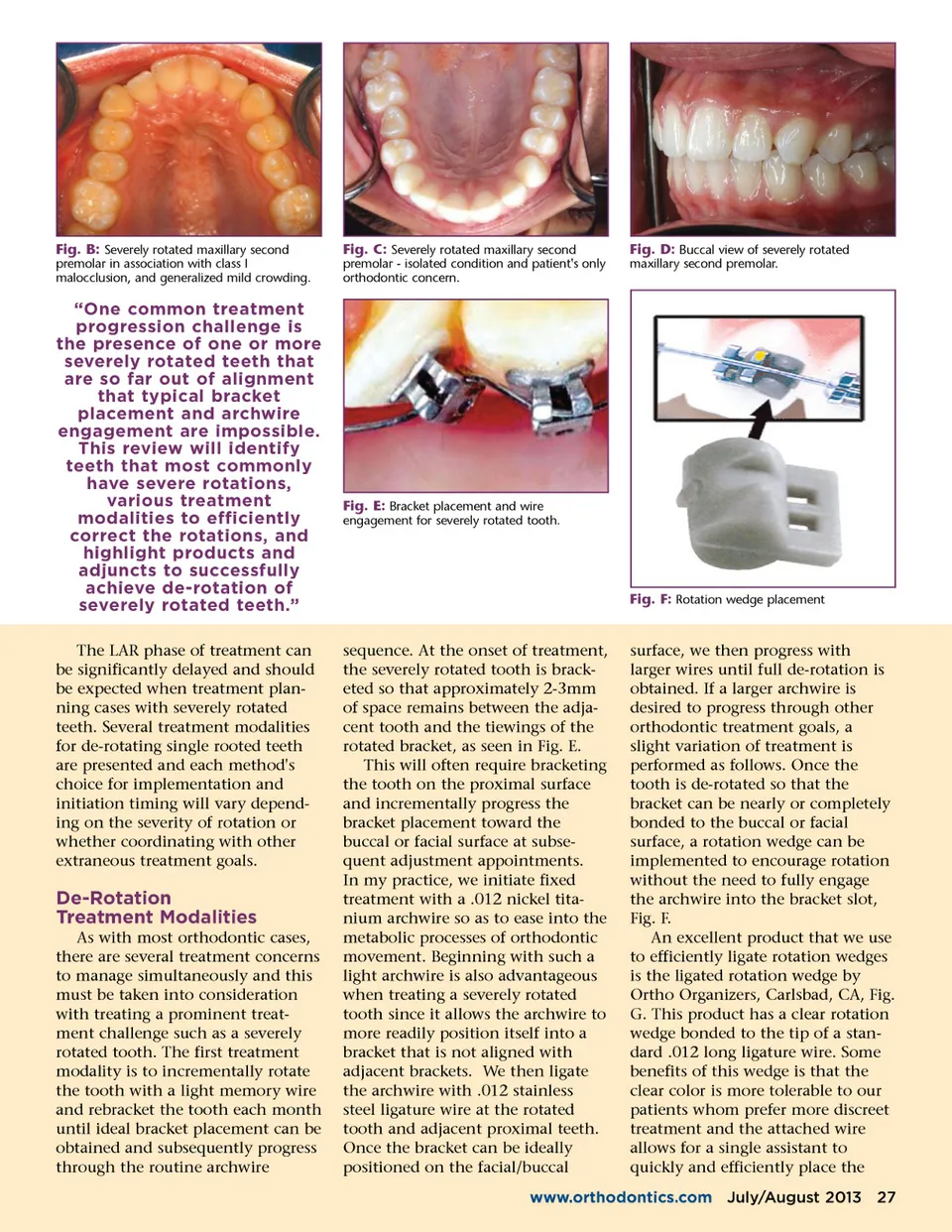
Fig. B: Severely rotated maxillary second premolar in association with class I malocclusion, and generalized mild crowding. Fig. C: Severely rotated maxillary second premolar -isolated condition and patient's only orthodontic concern. Fig. D: Buccal view of severely rotated maxillary second premolar. “One common treatment progression challenge is the presence of one or more severely rotated teeth that are so far out of alignment that typical bracket placement and archwire engagement are impossible. This review will identify teeth that most commonly have severe rotations, various treatment modalities to efficiently correct the rotations, and highlight products and adjuncts to successfully achieve de-rotation of severely rotated teeth.” The LAR phase of treatment can be significantly delayed and should be expected when treatment plan-ning cases with severely rotated teeth. Several treatment modalities for de-rotating single rooted teeth are presented and each method's choice for implementation and initiation timing will vary depend-ing on the severity of rotation or whether coordinating with other extraneous treatment goals. Fig. E: Bracket placement and wire engagement for severely rotated tooth. Fig. F: Rotation wedge placement De-Rotation Treatment Modalities As with most orthodontic cases, there are several treatment concerns to manage simultaneously and this must be taken into consideration with treating a prominent treat-ment challenge such as a severely rotated tooth. The first treatment modality is to incrementally rotate the tooth with a light memory wire and rebracket the tooth each month until ideal bracket placement can be obtained and subsequently progress through the routine archwire sequence. At the onset of treatment, the severely rotated tooth is brack-eted so that approximately 2-3mm of space remains between the adja-cent tooth and the tiewings of the rotated bracket, as seen in Fig. E. This will often require bracketing the tooth on the proximal surface and incrementally progress the bracket placement toward the buccal or facial surface at subse-quent adjustment appointments. In my practice, we initiate fixed treatment with a .012 nickel tita-nium archwire so as to ease into the metabolic processes of orthodontic movement. Beginning with such a light archwire is also advantageous when treating a severely rotated tooth since it allows the archwire to more readily position itself into a bracket that is not aligned with adjacent brackets. We then ligate the archwire with .012 stainless steel ligature wire at the rotated tooth and adjacent proximal teeth. Once the bracket can be ideally positioned on the facial/buccal surface, we then progress with larger wires until full de-rotation is obtained. If a larger archwire is desired to progress through other orthodontic treatment goals, a slight variation of treatment is performed as follows. Once the tooth is de-rotated so that the bracket can be nearly or completely bonded to the buccal or facial surface, a rotation wedge can be implemented to encourage rotation without the need to fully engage the archwire into the bracket slot, Fig. F. An excellent product that we use to efficiently ligate rotation wedges is the ligated rotation wedge by Ortho Organizers, Carlsbad, CA, Fig. G. This product has a clear rotation wedge bonded to the tip of a stan-dard .012 long ligature wire. Some benefits of this wedge is that the clear color is more tolerable to our patients whom prefer more discreet treatment and the attached wire allows for a single assistant to quickly and efficiently place the www.orthodontics.com July/August 2013 27
Journal of the American Orthodontic Society July-August 2013 Buyer's Guide: Page 27