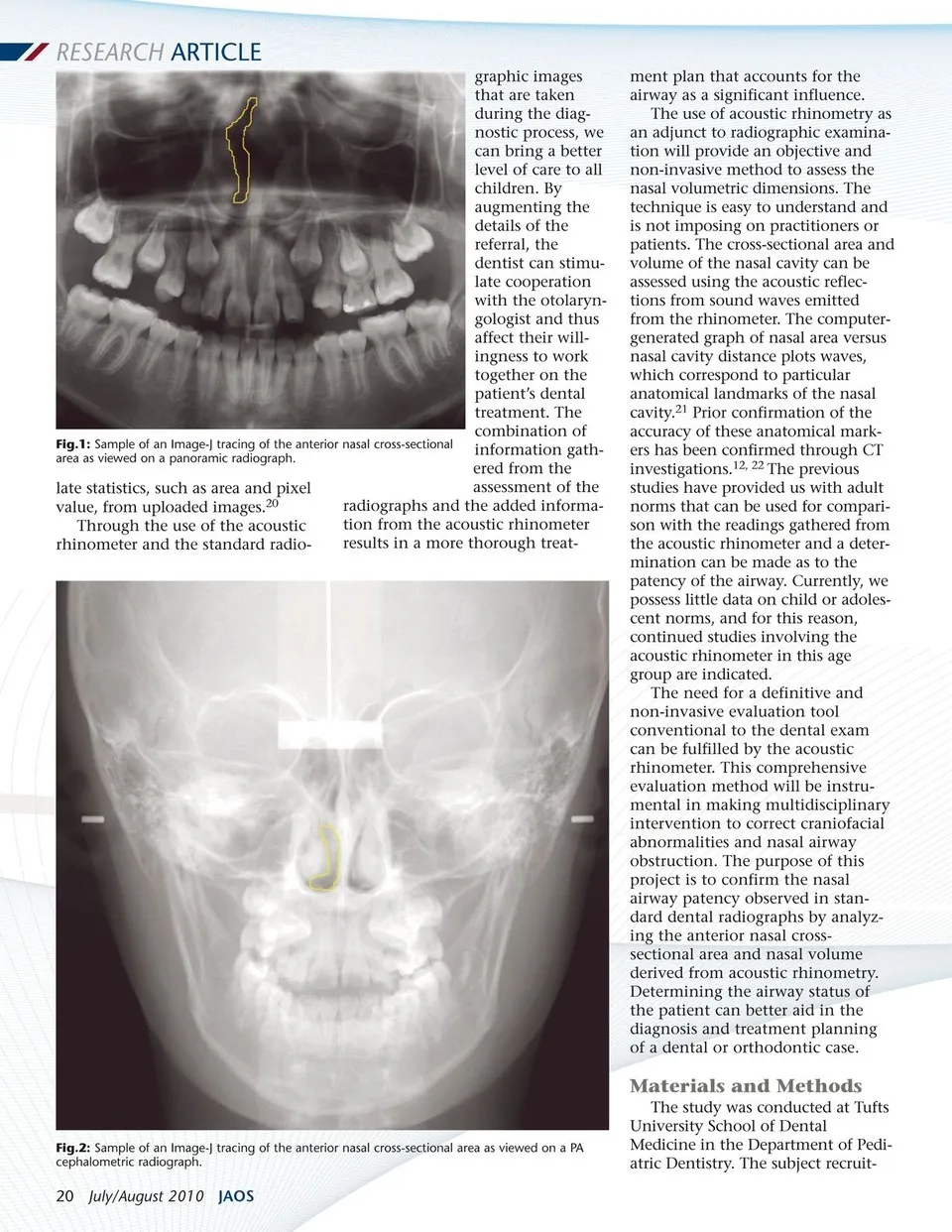
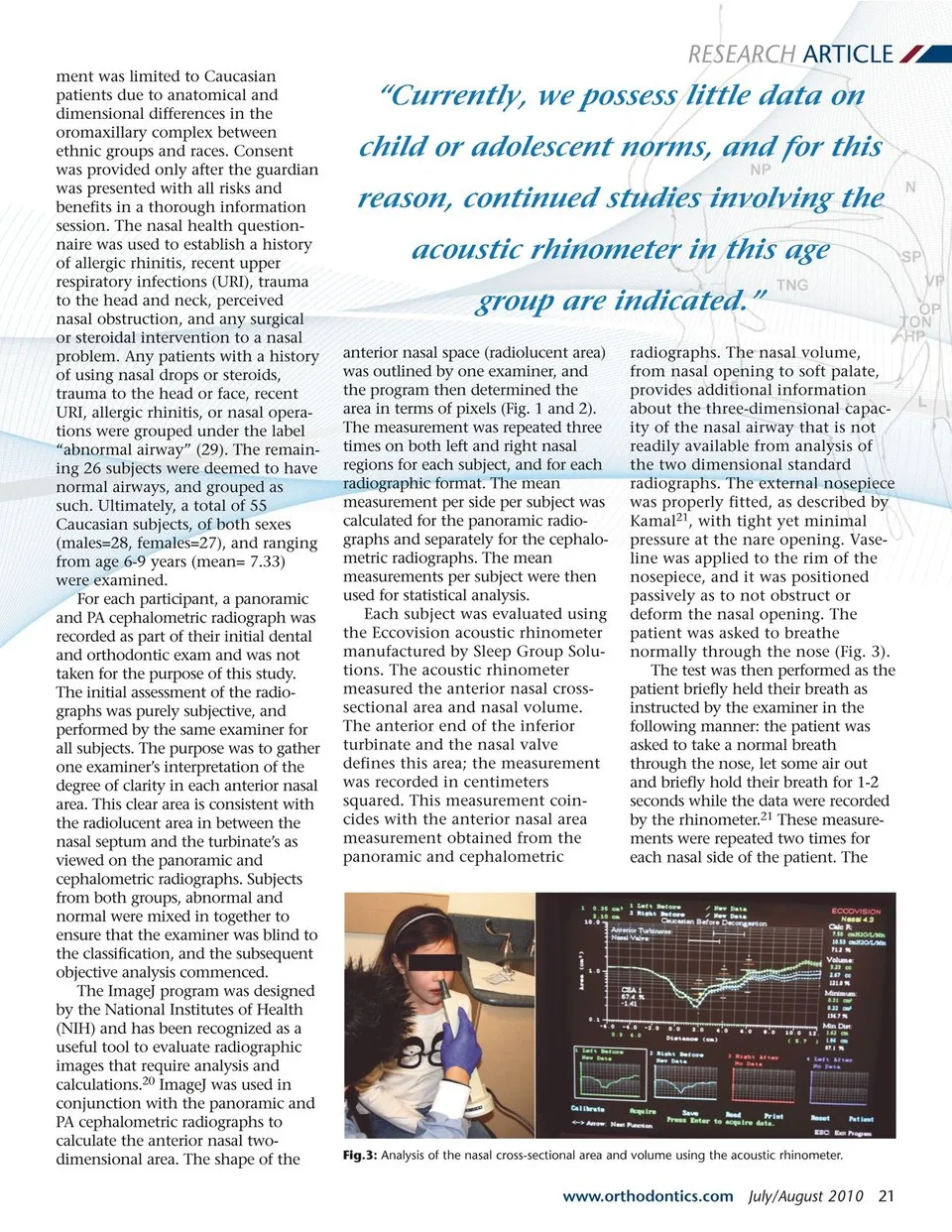
RESEARCH ARTICLE ment was limited to Caucasian patients due to anatomical and dimensional differences in the oromaxillary complex between ethnic groups and races. Consent was provided only after the guardian was presented with all risks and benefits in a thorough information session. The nasal health question-naire was used to establish a history of allergic rhinitis, recent upper respiratory infections (URI), trauma to the head and neck, perceived nasal obstruction, and any surgical or steroidal intervention to a nasal problem. Any patients with a history of using nasal drops or steroids, trauma to the head or face, recent URI, allergic rhinitis, or nasal opera-tions were grouped under the label “abnormal airway” (29). The remain-ing 26 subjects were deemed to have normal airways, and grouped as such. Ultimately, a total of 55 Caucasian subjects, of both sexes (males=28, females=27), and ranging from age 6-9 years (mean= 7.33) were examined. For each participant, a panoramic and PA cephalometric radiograph was recorded as part of their initial dental and orthodontic exam and was not taken for the purpose of this study. The initial assessment of the radio-graphs was purely subjective, and performed by the same examiner for all subjects. The purpose was to gather one examiner’s interpretation of the degree of clarity in each anterior nasal area. This clear area is consistent with the radiolucent area in between the nasal septum and the turbinate’s as viewed on the panoramic and cephalometric radiographs. Subjects from both groups, abnormal and normal were mixed in together to ensure that the examiner was blind to the classification, and the subsequent objective analysis commenced. The ImageJ program was designed by the National Institutes of Health (NIH) and has been recognized as a useful tool to evaluate radiographic images that require analysis and calculations.20 ImageJ was used in conjunction with the panoramic and PA cephalometric radiographs to calculate the anterior nasal two-dimensional area. The shape of the “Currently, we possess little data on child or adolescent norms, and for this reason, continued studies involving the acoustic rhinometer in this age group are indicated.” anterior nasal space (radiolucent area) was outlined by one examiner, and the program then determined the area in terms of pixels (Fig. 1 and 2). The measurement was repeated three times on both left and right nasal regions for each subject, and for each radiographic format. The mean measurement per side per subject was calculated for the panoramic radio-graphs and separately for the cephalo-metric radiographs. The mean measurements per subject were then used for statistical analysis. Each subject was evaluated using the Eccovision acoustic rhinometer manufactured by Sleep Group Solu-tions. The acoustic rhinometer measured the anterior nasal cross-sectional area and nasal volume. The anterior end of the inferior turbinate and the nasal valve defines this area; the measurement was recorded in centimeters squared. This measurement coin-cides with the anterior nasal area measurement obtained from the panoramic and cephalometric radiographs. The nasal volume, from nasal opening to soft palate, provides additional information about the three-dimensional capac-ity of the nasal airway that is not readily available from analysis of the two dimensional standard radiographs. The external nosepiece was properly fitted, as described by Kamal21, with tight yet minimal pressure at the nare opening. Vase-line was applied to the rim of the nosepiece, and it was positioned passively as to not obstruct or deform the nasal opening. The patient was asked to breathe normally through the nose (Fig. 3). The test was then performed as the patient briefly held their breath as instructed by the examiner in the following manner: the patient was asked to take a normal breath through the nose, let some air out and briefly hold their breath for 1-2 seconds while the data were recorded by the rhinometer.21 These measure-ments were repeated two times for each nasal side of the patient. The Fig.3: Analysis of the nasal cross-sectional area and volume using the acoustic rhinometer. www.orthodontics.com July/August 2010 21
Journal of the American Orthodontic Society July-August 2010/Buyer's Guide: Page 21