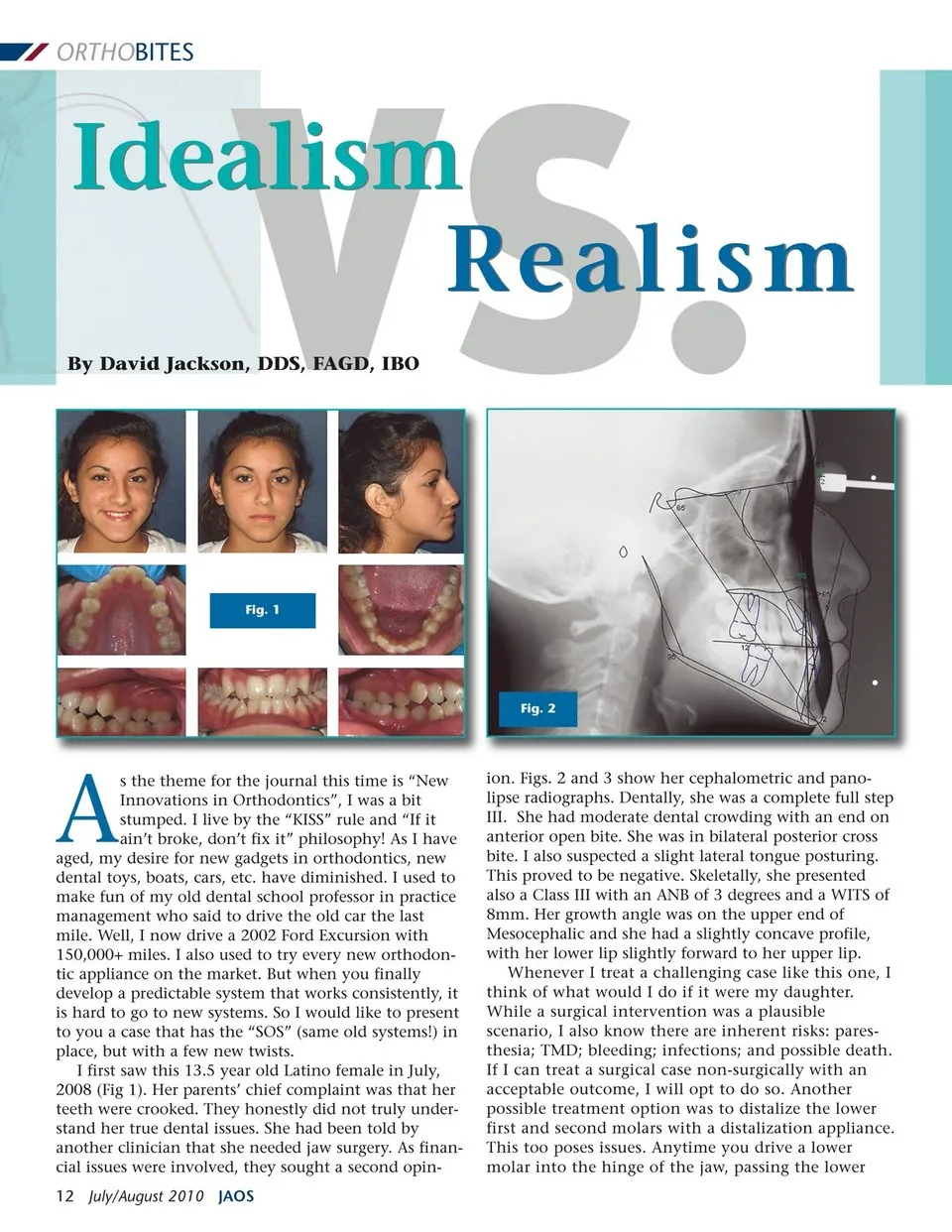
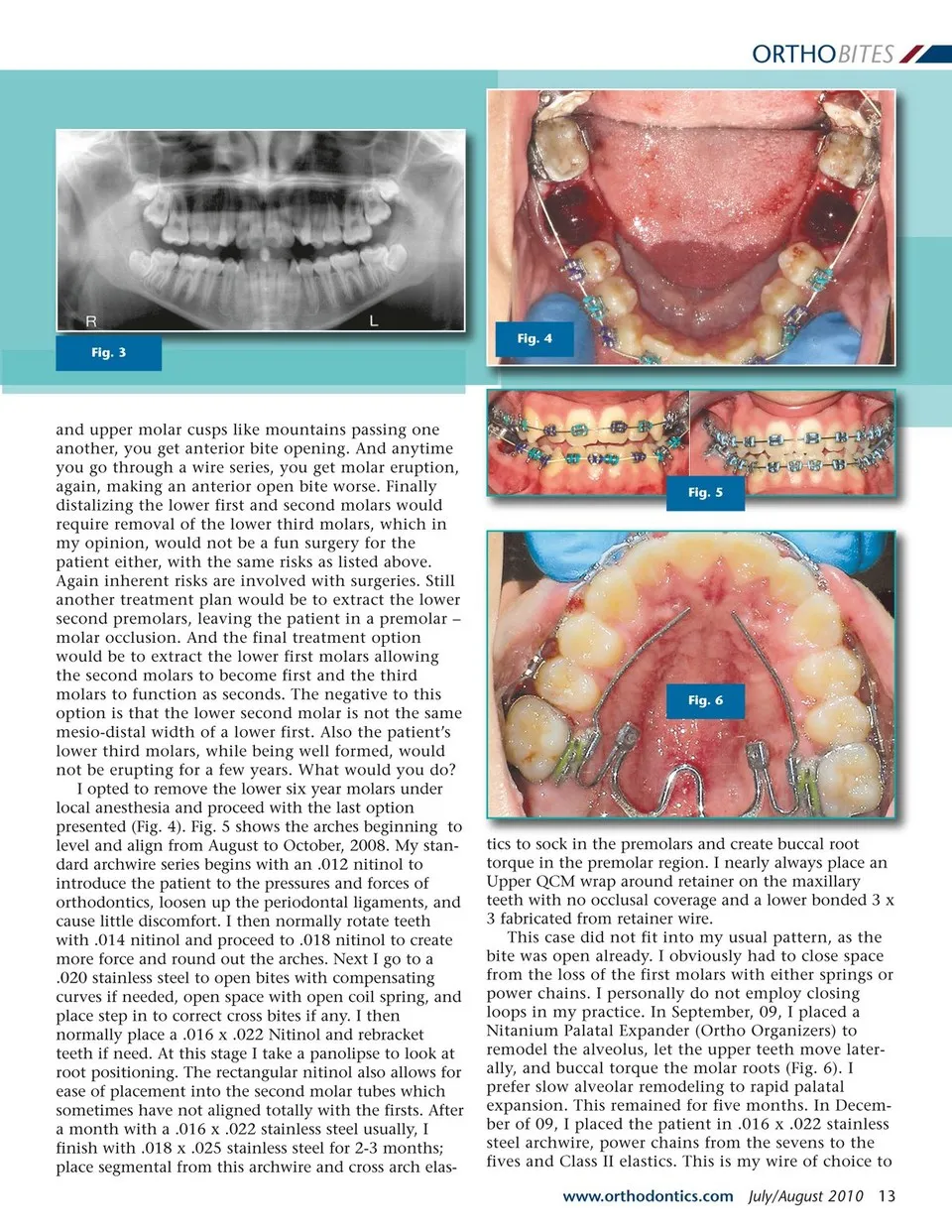
ORTHOBITES Fig. 4 Fig. 3 and upper molar cusps like mountains passing one another, you get anterior bite opening. And anytime you go through a wire series, you get molar eruption, again, making an anterior open bite worse. Finally distalizing the lower first and second molars would require removal of the lower third molars, which in my opinion, would not be a fun surgery for the patient either, with the same risks as listed above. Again inherent risks are involved with surgeries. Still another treatment plan would be to extract the lower second premolars, leaving the patient in a premolar – molar occlusion. And the final treatment option would be to extract the lower first molars allowing the second molars to become first and the third molars to function as seconds. The negative to this option is that the lower second molar is not the same mesio-distal width of a lower first. Also the patient’s lower third molars, while being well formed, would not be erupting for a few years. What would you do? I opted to remove the lower six year molars under local anesthesia and proceed with the last option presented (Fig. 4). Fig. 5 shows the arches beginning to level and align from August to October, 2008. My stan-dard archwire series begins with an .012 nitinol to introduce the patient to the pressures and forces of orthodontics, loosen up the periodontal ligaments, and cause little discomfort. I then normally rotate teeth with .014 nitinol and proceed to .018 nitinol to create more force and round out the arches. Next I go to a .020 stainless steel to open bites with compensating curves if needed, open space with open coil spring, and place step in to correct cross bites if any. I then normally place a .016 x .022 Nitinol and rebracket teeth if need. At this stage I take a panolipse to look at root positioning. The rectangular nitinol also allows for ease of placement into the second molar tubes which sometimes have not aligned totally with the firsts. After a month with a .016 x .022 stainless steel usually, I finish with .018 x .025 stainless steel for 2-3 months; place segmental from this archwire and cross arch elas-Fig. 5 Fig. 6 tics to sock in the premolars and create buccal root torque in the premolar region. I nearly always place an Upper QCM wrap around retainer on the maxillary teeth with no occlusal coverage and a lower bonded 3 x 3 fabricated from retainer wire. This case did not fit into my usual pattern, as the bite was open already. I obviously had to close space from the loss of the first molars with either springs or power chains. I personally do not employ closing loops in my practice. In September, 09, I placed a Nitanium Palatal Expander (Ortho Organizers) to remodel the alveolus, let the upper teeth move later-ally, and buccal torque the molar roots (Fig. 6). I prefer slow alveolar remodeling to rapid palatal expansion. This remained for five months. In Decem-ber of 09, I placed the patient in .016 x .022 stainless steel archwire, power chains from the sevens to the fives and Class II elastics. This is my wire of choice to www.orthodontics.com July/August 2010 13
Journal of the American Orthodontic Society July-August 2010/Buyer's Guide: Page 13