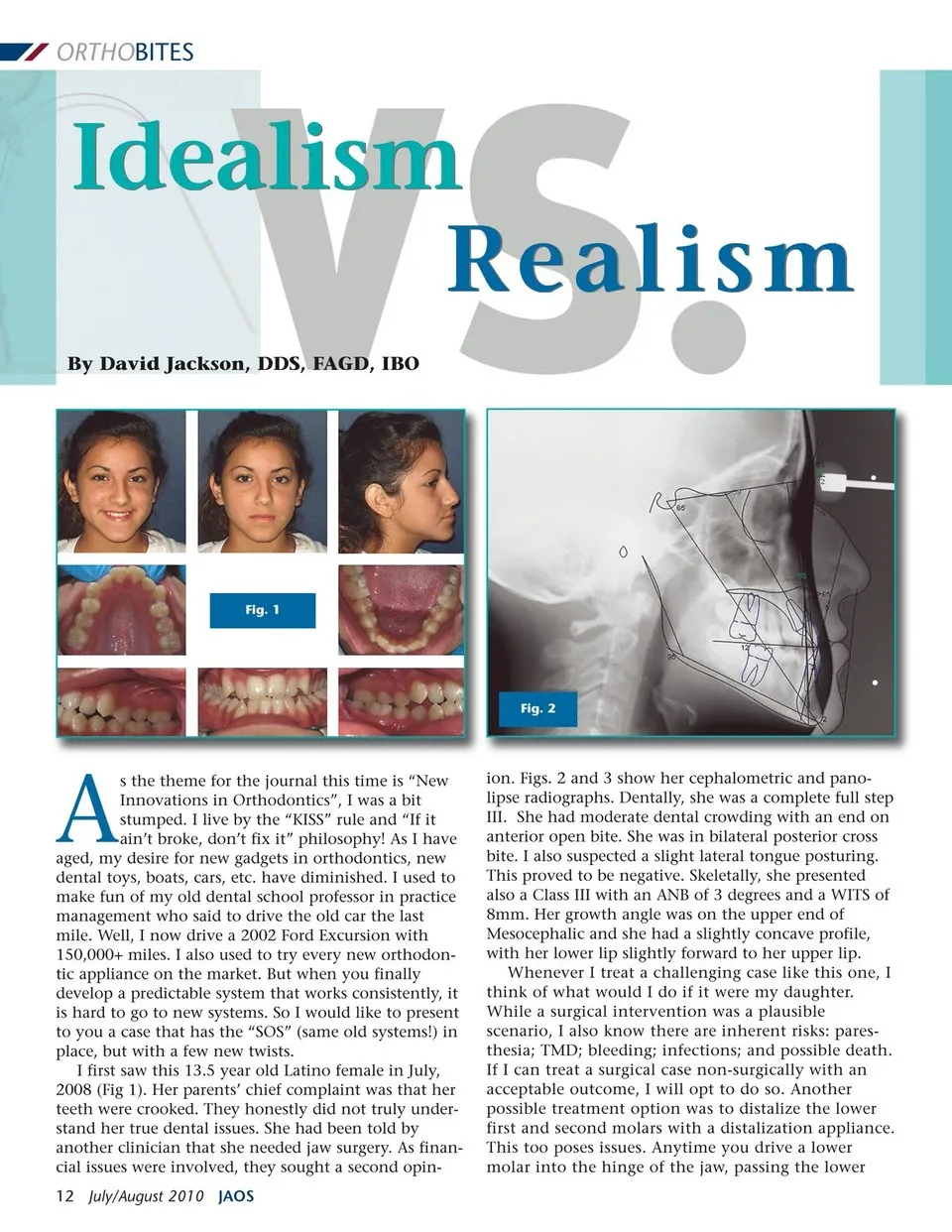
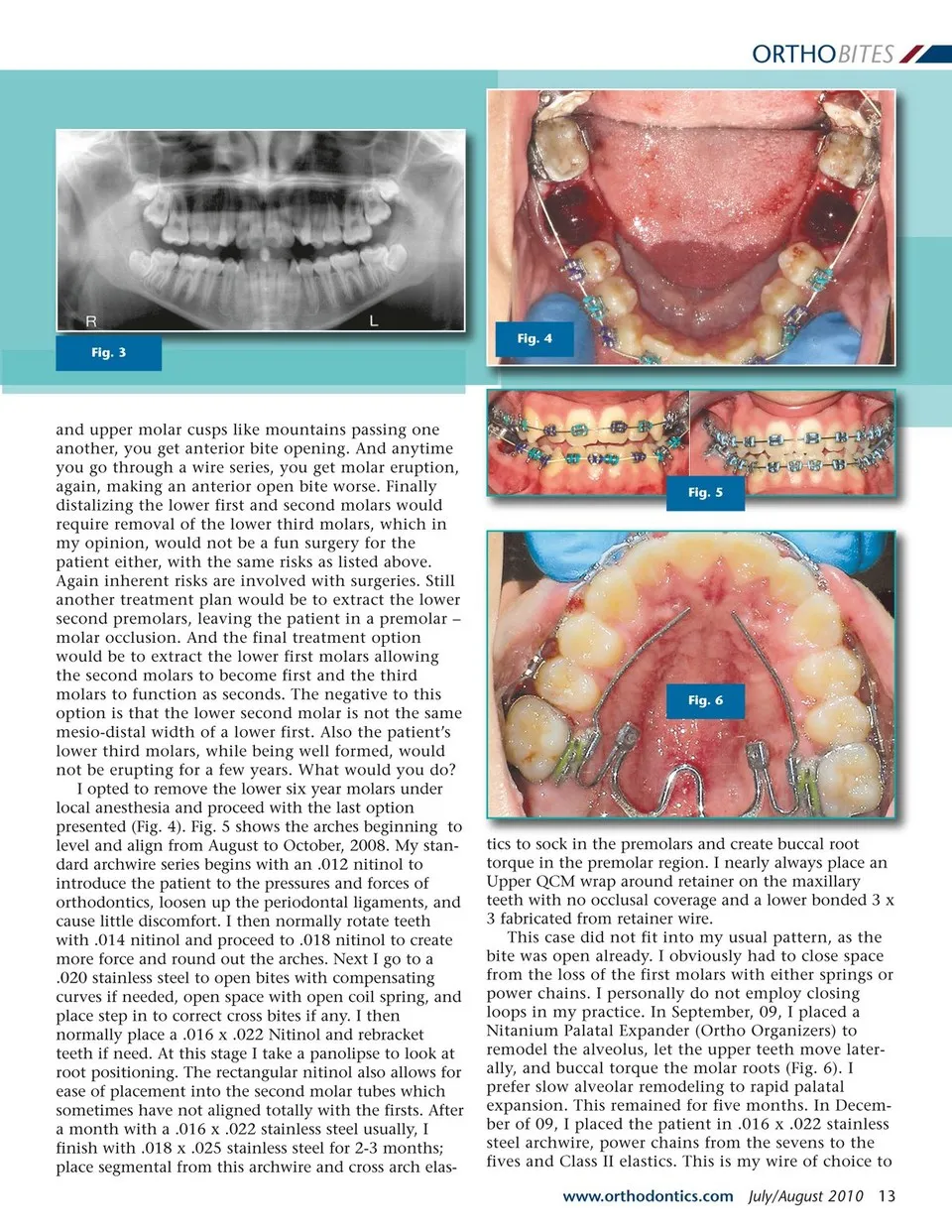
ORTHOBITES Idealism By David Jackson, DDS, FAGD, IBO VS. Fig. 1 Fig. 2 A s the theme for the journal this time is “New Innovations in Orthodontics”, I was a bit stumped. I live by the “KISS” rule and “If it ain’t broke, don’t fix it” philosophy! As I have aged, my desire for new gadgets in orthodontics, new dental toys, boats, cars, etc. have diminished. I used to make fun of my old dental school professor in practice management who said to drive the old car the last mile. Well, I now drive a 2002 Ford Excursion with 150,000+ miles. I also used to try every new orthodon-tic appliance on the market. But when you finally develop a predictable system that works consistently, it is hard to go to new systems. So I would like to present to you a case that has the “SOS” (same old systems!) in place, but with a few new twists. I first saw this 13.5 year old Latino female in July, 2008 (Fig 1). Her parents’ chief complaint was that her teeth were crooked. They honestly did not truly under-stand her true dental issues. She had been told by another clinician that she needed jaw surgery. As finan-cial issues were involved, they sought a second opin-12 July/August 2010 JAOS Realism ion. Figs. 2 and 3 show her cephalometric and pano-lipse radiographs. Dentally, she was a complete full step III. She had moderate dental crowding with an end on anterior open bite. She was in bilateral posterior cross bite. I also suspected a slight lateral tongue posturing. This proved to be negative. Skeletally, she presented also a Class III with an ANB of 3 degrees and a WITS of 8mm. Her growth angle was on the upper end of Mesocephalic and she had a slightly concave profile, with her lower lip slightly forward to her upper lip. Whenever I treat a challenging case like this one, I think of what would I do if it were my daughter. While a surgical intervention was a plausible scenario, I also know there are inherent risks: pares-thesia; TMD; bleeding; infections; and possible death. If I can treat a surgical case non-surgically with an acceptable outcome, I will opt to do so. Another possible treatment option was to distalize the lower first and second molars with a distalization appliance. This too poses issues. Anytime you drive a lower molar into the hinge of the jaw, passing the lower
Journal of the American Orthodontic Society July-August 2010/Buyer's Guide: Page 12