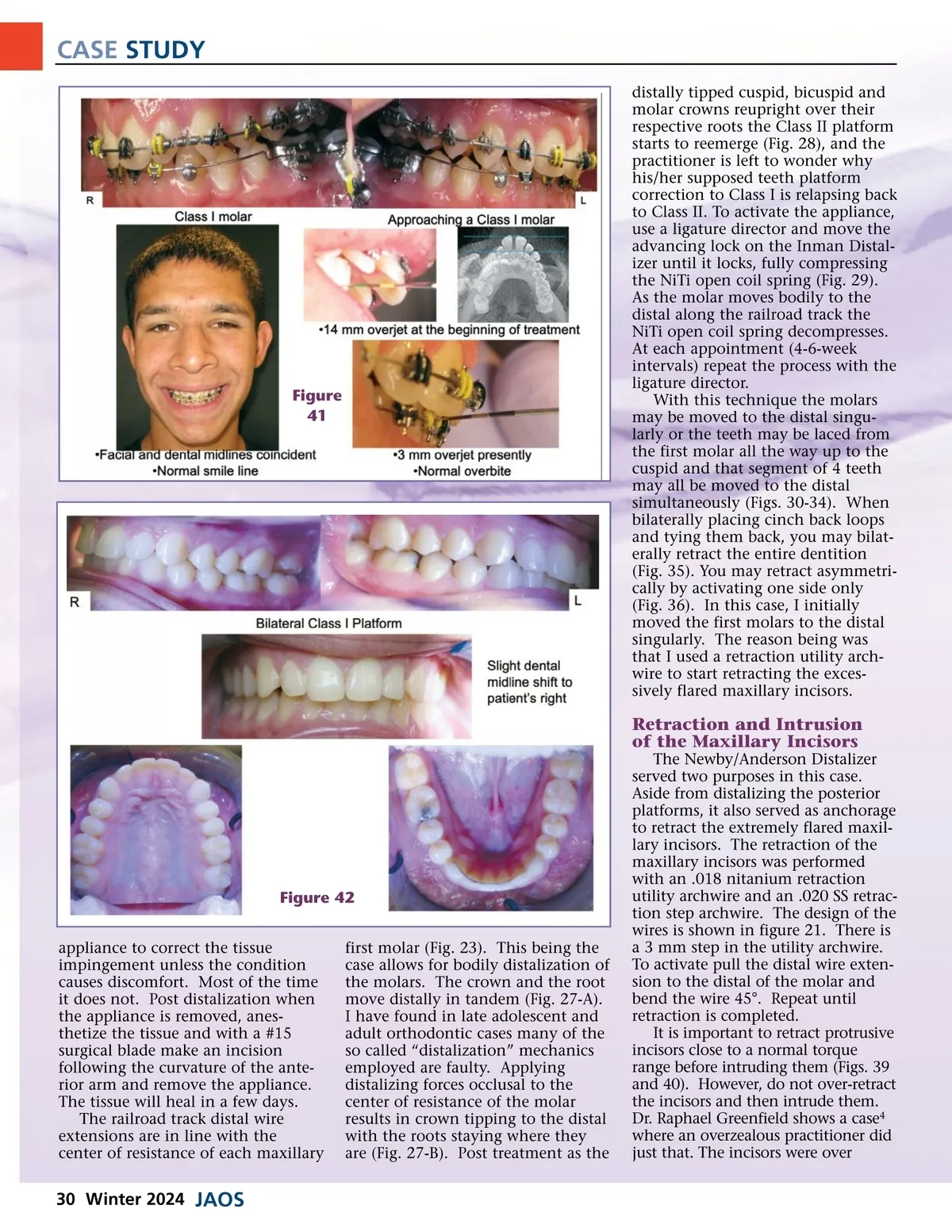
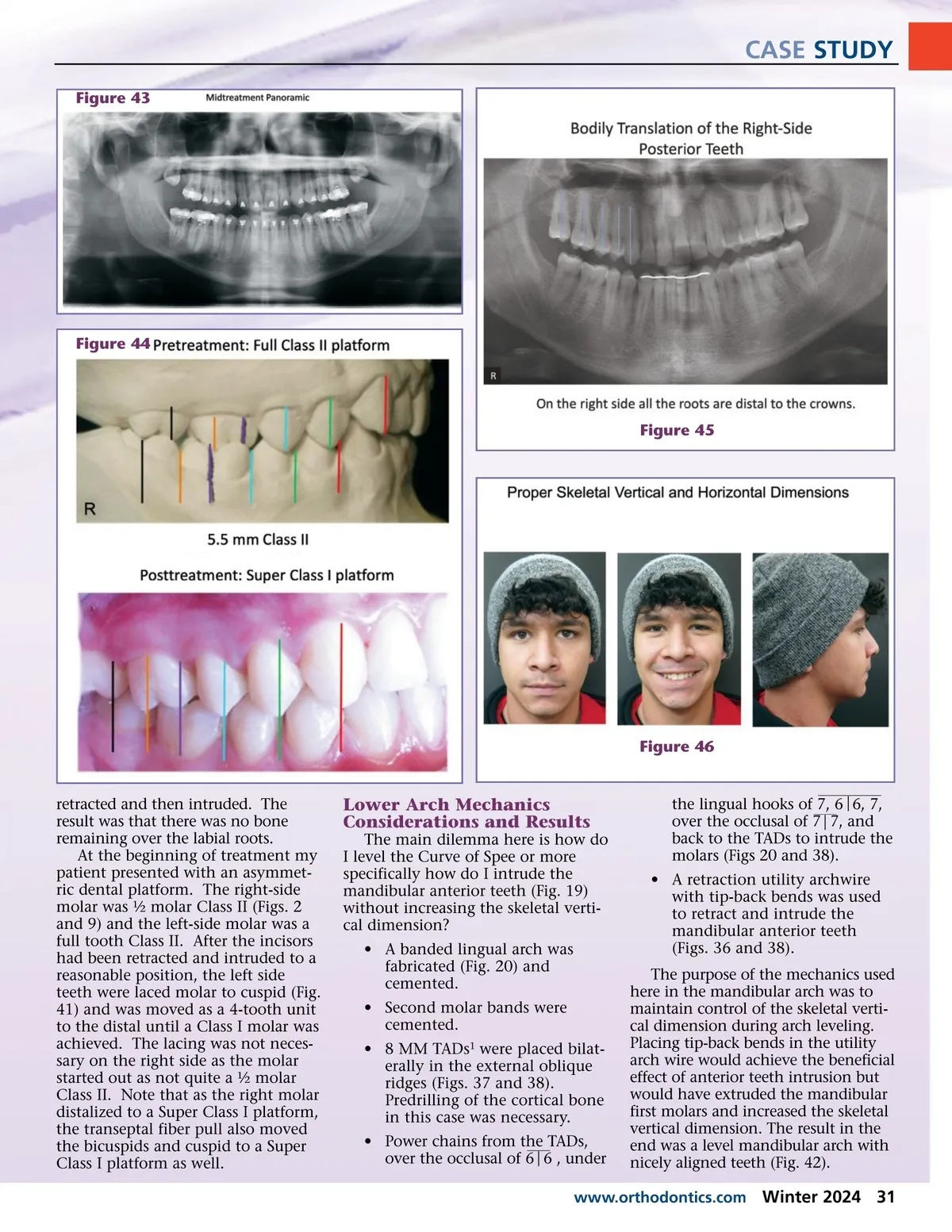
CASE STUDY distally tipped cuspid, bicuspid and molar crowns reupright over their respective roots the Class II platform starts to reemerge (Fig. 28), and the practitioner is left to wonder why his/her supposed teeth platform correction to Class I is relapsing back to Class II. To activate the appliance, use a ligature director and move the advancing lock on the Inman Distal-izer until it locks, fully compressing the NiTi open coil spring (Fig. 29). As the molar moves bodily to the distal along the railroad track the NiTi open coil spring decompresses. At each appointment (4-6-week intervals) repeat the process with the ligature director. With this technique the molars may be moved to the distal singu-larly or the teeth may be laced from the first molar all the way up to the cuspid and that segment of 4 teeth may all be moved to the distal simultaneously (Figs. 30-34). When bilaterally placing cinch back loops and tying them back, you may bilat-erally retract the entire dentition (Fig. 35). You may retract asymmetri-cally by activating one side only (Fig. 36). In this case, I initially moved the first molars to the distal singularly. The reason being was that I used a retraction utility arch-wire to start retracting the exces-sively flared maxillary incisors. Figure 41 Retraction and Intrusion of the Maxillary Incisors The Newby/Anderson Distalizer served two purposes in this case. Aside from distalizing the posterior platforms, it also served as anchorage to retract the extremely flared maxil-lary incisors. The retraction of the maxillary incisors was performed with an .018 nitanium retraction utility archwire and an .020 SS retrac-tion step archwire. The design of the wires is shown in figure 21. There is a 3 mm step in the utility archwire. To activate pull the distal wire exten-sion to the distal of the molar and bend the wire 45°. Repeat until retraction is completed. It is important to retract protrusive incisors close to a normal torque range before intruding them (Figs. 39 and 40). However, do not over-retract the incisors and then intrude them. Dr. Raphael Greenfield shows a case 4 where an overzealous practitioner did just that. The incisors were over Figure 42 appliance to correct the tissue impingement unless the condition causes discomfort. Most of the time it does not. Post distalization when the appliance is removed, anes-thetize the tissue and with a #15 surgical blade make an incision following the curvature of the ante-rior arm and remove the appliance. The tissue will heal in a few days. The railroad track distal wire extensions are in line with the center of resistance of each maxillary first molar (Fig. 23). This being the case allows for bodily distalization of the molars. The crown and the root move distally in tandem (Fig. 27-A). I have found in late adolescent and adult orthodontic cases many of the so called “distalization” mechanics employed are faulty. Applying distalizing forces occlusal to the center of resistance of the molar results in crown tipping to the distal with the roots staying where they are (Fig. 27-B). Post treatment as the 30 Winter 2024 JAOS
Journal of the American Orthodontic Society JAOS Winter 2024: Page 30