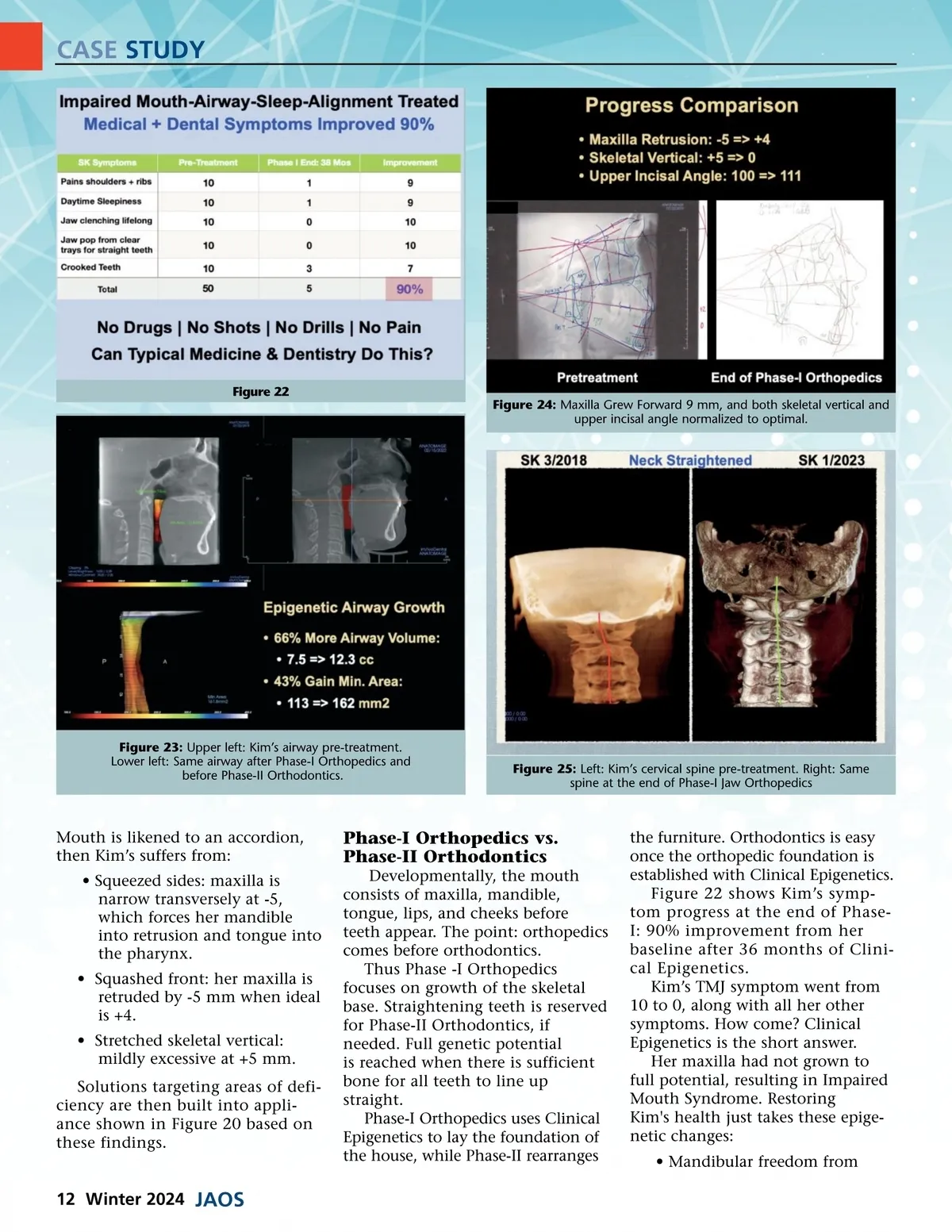
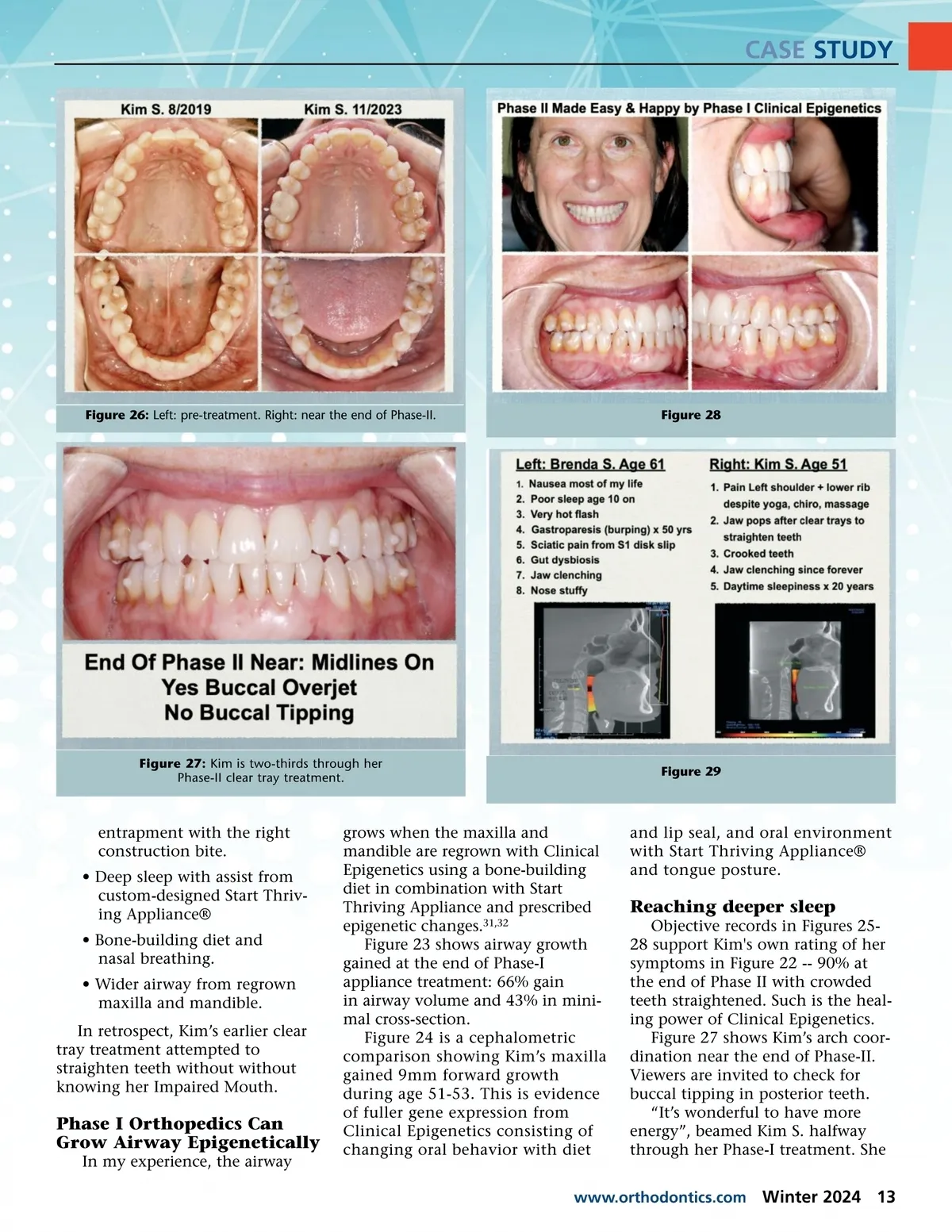
CASE STUDY Figure 22 Figure 24: Maxilla Grew Forward 9 mm, and both skeletal vertical and upper incisal angle normalized to optimal. Figure 23: Upper left: Kim’s airway pre-treatment. Lower left: Same airway after Phase-I Orthopedics and before Phase-II Orthodontics. Figure 25: Left: Kim’s cervical spine pre-treatment. Right: Same spine at the end of Phase-I Jaw Orthopedics Mouth is likened to an accordion, then Kim’s suffers from: • Squeezed sides: maxilla is narrow transversely at -5, which forces her mandible into retrusion and tongue into the pharynx. • Squashed front: her maxilla is retruded by -5 mm when ideal is +4. • Stretched skeletal vertical: mildly excessive at +5 mm. Solutions targeting areas of defi-ciency are then built into appli-ance shown in Figure 20 based on these findings. Phase-I Orthopedics vs. Phase-II Orthodontics Developmentally, the mouth consists of maxilla, mandible, tongue, lips, and cheeks before teeth appear. The point: orthopedics comes before orthodontics. Thus Phase -I Orthopedics focuses on growth of the skeletal base. Straightening teeth is reserved for Phase-II Orthodontics, if needed. Full genetic potential is reached when there is sufficient bone for all teeth to line up straight. Phase-I Orthopedics uses Clinical Epigenetics to lay the foundation of the house, while Phase-II rearranges the furniture. Orthodontics is easy once the orthopedic foundation is established with Clinical Epigenetics. Figure 22 shows Kim’s symp-tom progress at the end of Phase-I: 90% improvement from her baseline after 36 months of Clini-cal Epigenetics. Kim’s TMJ symptom went from 10 to 0, along with all her other symptoms. How come? Clinical Epigenetics is the short answer. Her maxilla had not grown to full potential, resulting in Impaired Mouth Syndrome. Restoring Kim's health just takes these epige-netic changes: • Mandibular freedom from 12 Winter 2024 JAOS
Journal of the American Orthodontic Society JAOS Winter 2024: Page 12