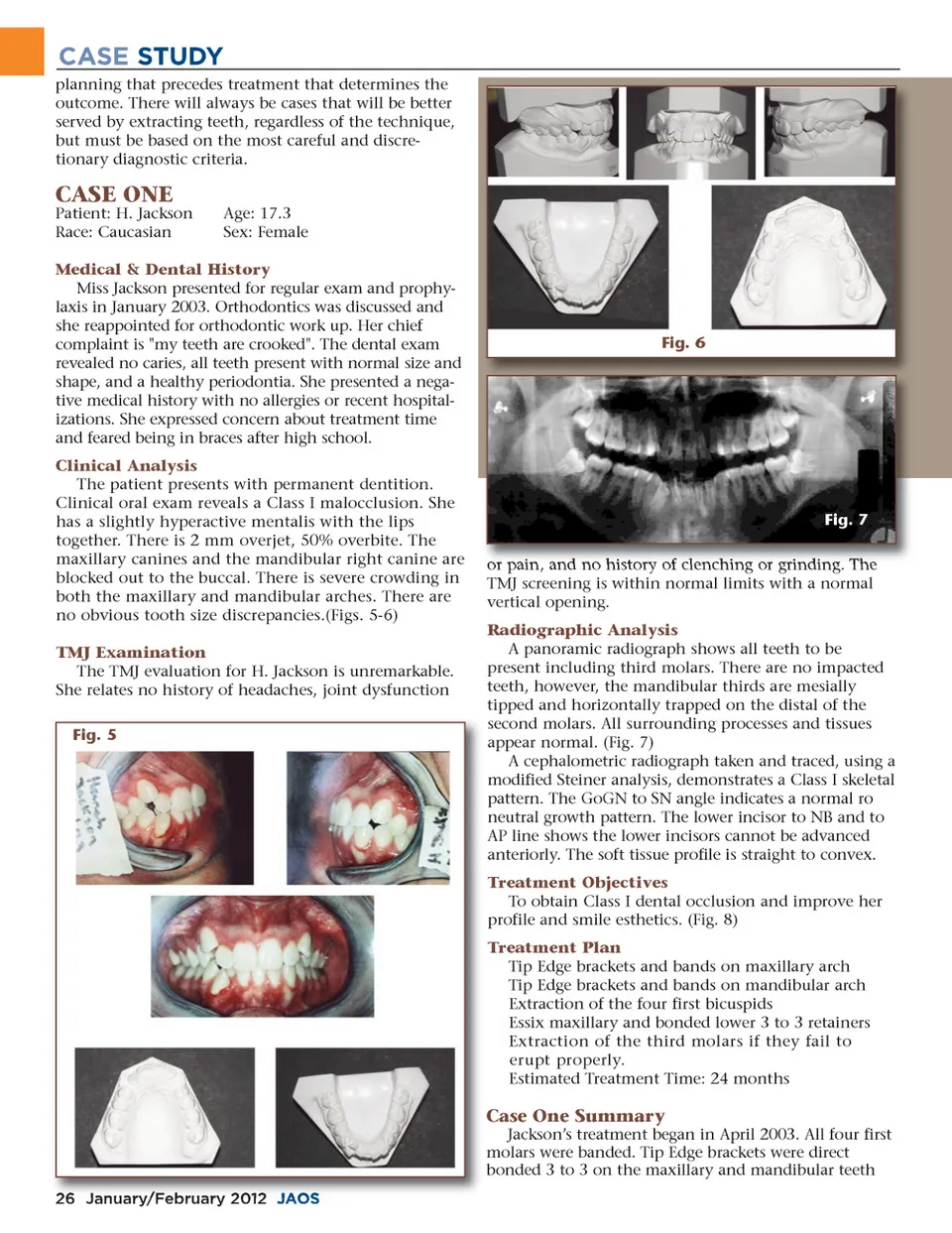
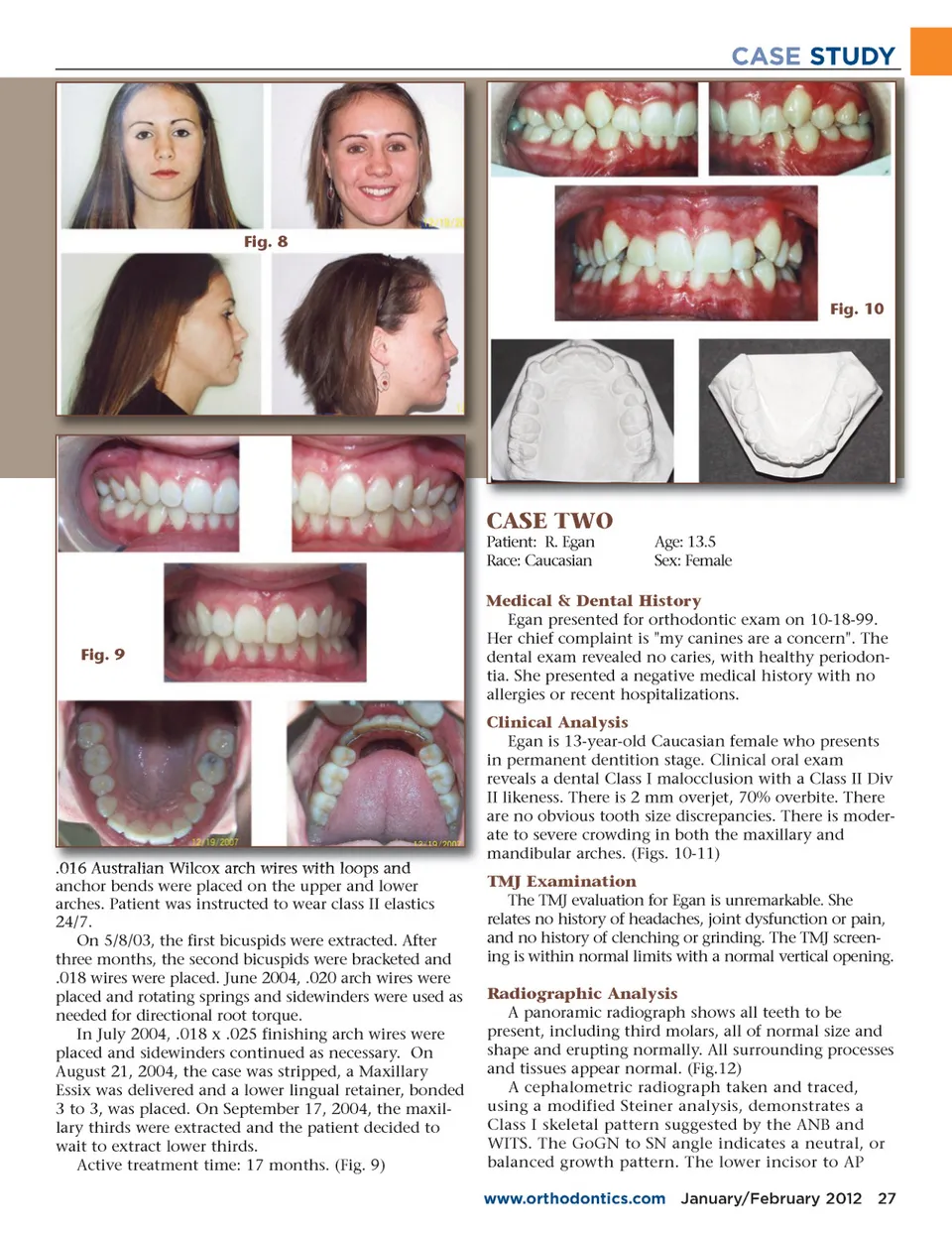
CASE STUDY planning that precedes treatment that determines the outcome. There will always be cases that will be better served by extracting teeth, regardless of the technique, but must be based on the most careful and discre-tionary diagnostic criteria. CASE ONE Patient: H. Jackson Race: Caucasian Age: 17.3 Sex: Female Medical & Dental History Miss Jackson presented for regular exam and prophy-laxis in January 2003. Orthodontics was discussed and she reappointed for orthodontic work up. Her chief complaint is "my teeth are crooked". The dental exam revealed no caries, all teeth present with normal size and shape, and a healthy periodontia. She presented a nega-tive medical history with no allergies or recent hospital-izations. She expressed concern about treatment time and feared being in braces after high school. Clinical Analysis The patient presents with permanent dentition. Clinical oral exam reveals a Class I malocclusion. She has a slightly hyperactive mentalis with the lips together. There is 2 mm overjet, 50% overbite. The maxillary canines and the mandibular right canine are blocked out to the buccal. There is severe crowding in both the maxillary and mandibular arches. There are no obvious tooth size discrepancies.(Figs. 5-6) TMJ Examination The TMJ evaluation for H. Jackson is unremarkable. She relates no history of headaches, joint dysfunction Fig. 5 Fig. 6 Fig. 7 or pain, and no history of clenching or grinding. The TMJ screening is within normal limits with a normal vertical opening. Radiographic Analysis A panoramic radiograph shows all teeth to be present including third molars. There are no impacted teeth, however, the mandibular thirds are mesially tipped and horizontally trapped on the distal of the second molars. All surrounding processes and tissues appear normal. (Fig. 7) A cephalometric radiograph taken and traced, using a modified Steiner analysis, demonstrates a Class I skeletal pattern. The GoGN to SN angle indicates a normal ro neutral growth pattern. The lower incisor to NB and to AP line shows the lower incisors cannot be advanced anteriorly. The soft tissue profile is straight to convex. Treatment Objectives To obtain Class I dental occlusion and improve her profile and smile esthetics. (Fig. 8) Treatment Plan Tip Edge brackets and bands on maxillary arch Tip Edge brackets and bands on mandibular arch Extraction of the four first bicuspids Essix maxillary and bonded lower 3 to 3 retainers Extraction of the third molars if they fail to erupt properly. Estimated Treatment Time: 24 months Case One Summary Jackson’s treatment began in April 2003. All four first molars were banded. Tip Edge brackets were direct bonded 3 to 3 on the maxillary and mandibular teeth 26 January/February 2012 JAOS
Journal of the American Orthodontic Society January-February 2012: Page 26