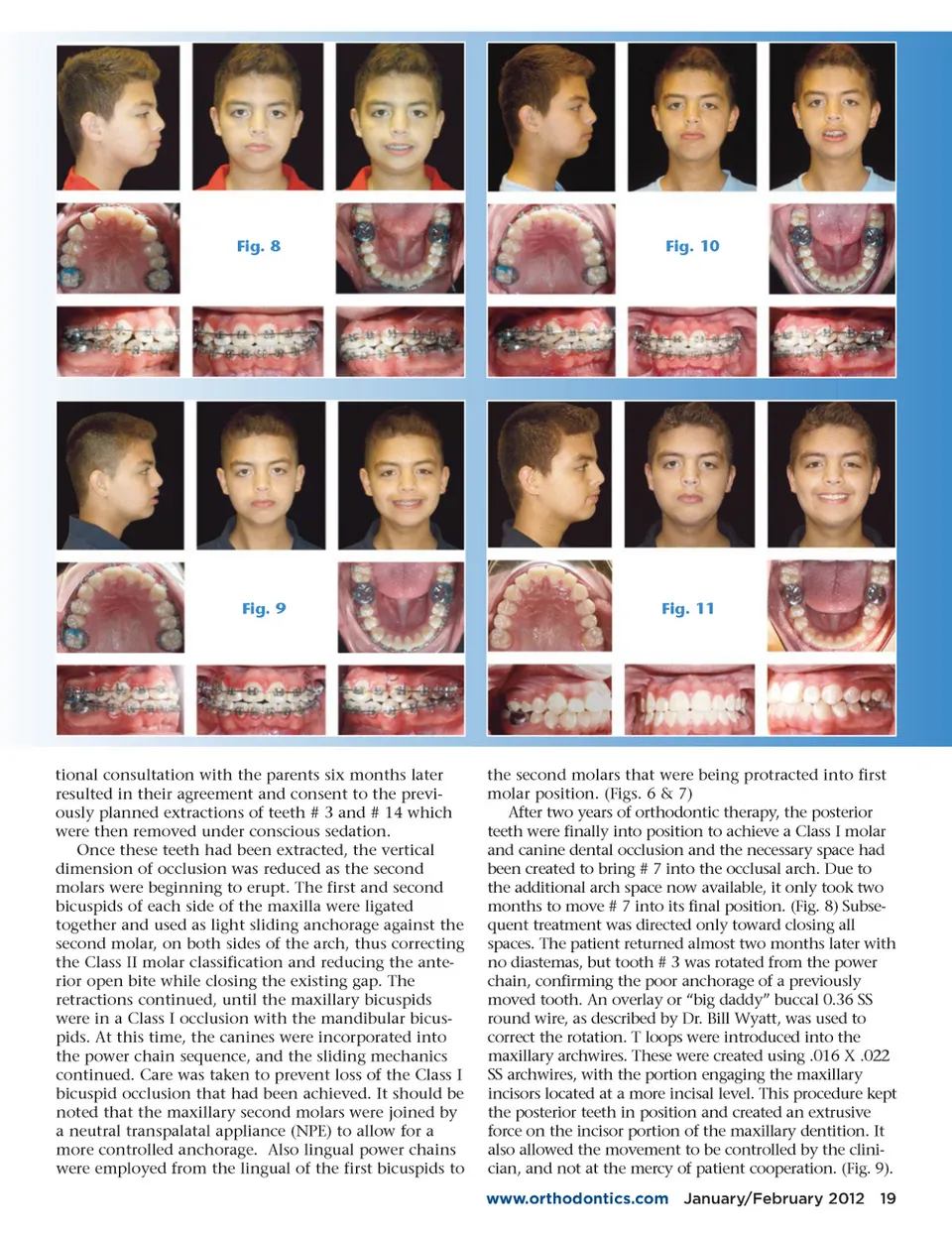
Fig. 8 Fig. 10 Fig. 9 Fig. 11 tional consultation with the parents six months later resulted in their agreement and consent to the previ-ously planned extractions of teeth # 3 and # 14 which were then removed under conscious sedation. Once these teeth had been extracted, the vertical dimension of occlusion was reduced as the second molars were beginning to erupt. The first and second bicuspids of each side of the maxilla were ligated together and used as light sliding anchorage against the second molar, on both sides of the arch, thus correcting the Class II molar classification and reducing the ante-rior open bite while closing the existing gap. The retractions continued, until the maxillary bicuspids were in a Class I occlusion with the mandibular bicus-pids. At this time, the canines were incorporated into the power chain sequence, and the sliding mechanics continued. Care was taken to prevent loss of the Class I bicuspid occlusion that had been achieved. It should be noted that the maxillary second molars were joined by a neutral transpalatal appliance (NPE) to allow for a more controlled anchorage. Also lingual power chains were employed from the lingual of the first bicuspids to the second molars that were being protracted into first molar position. (Figs. 6 & 7) After two years of orthodontic therapy, the posterior teeth were finally into position to achieve a Class I molar and canine dental occlusion and the necessary space had been created to bring # 7 into the occlusal arch. Due to the additional arch space now available, it only took two months to move # 7 into its final position. (Fig. 8) Subse-quent treatment was directed only toward closing all spaces. The patient returned almost two months later with no diastemas, but tooth # 3 was rotated from the power chain, confirming the poor anchorage of a previously moved tooth. An overlay or “big daddy” buccal 0.36 SS round wire, as described by Dr. Bill Wyatt, was used to correct the rotation. T loops were introduced into the maxillary archwires. These were created using .016 X .022 SS archwires, with the portion engaging the maxillary incisors located at a more incisal level. This procedure kept the posterior teeth in position and created an extrusive force on the incisor portion of the maxillary dentition. It also allowed the movement to be controlled by the clini-cian, and not at the mercy of patient cooperation. (Fig. 9). www.orthodontics.com January/February 2012 19
Journal of the American Orthodontic Society January-February 2012: Page 19