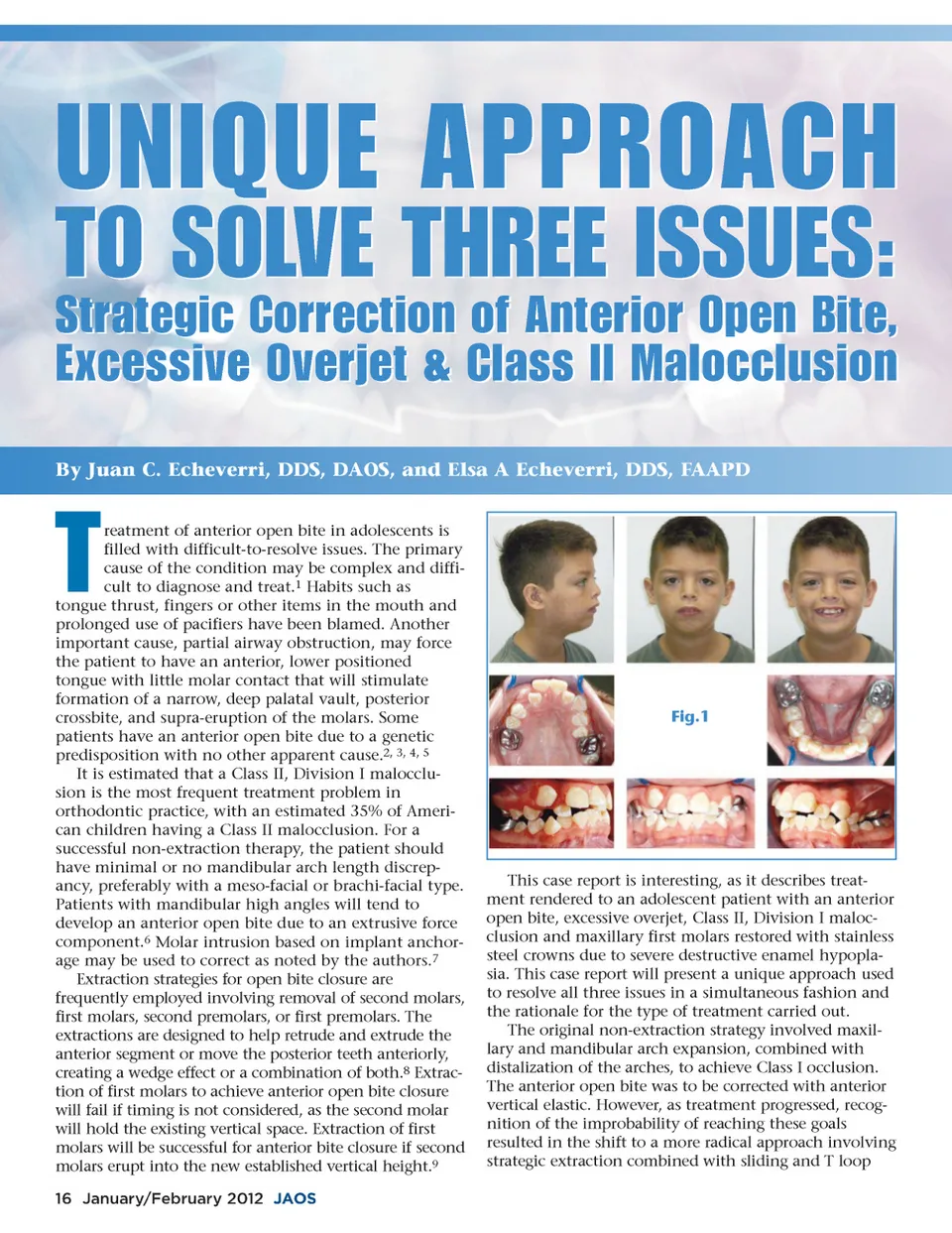
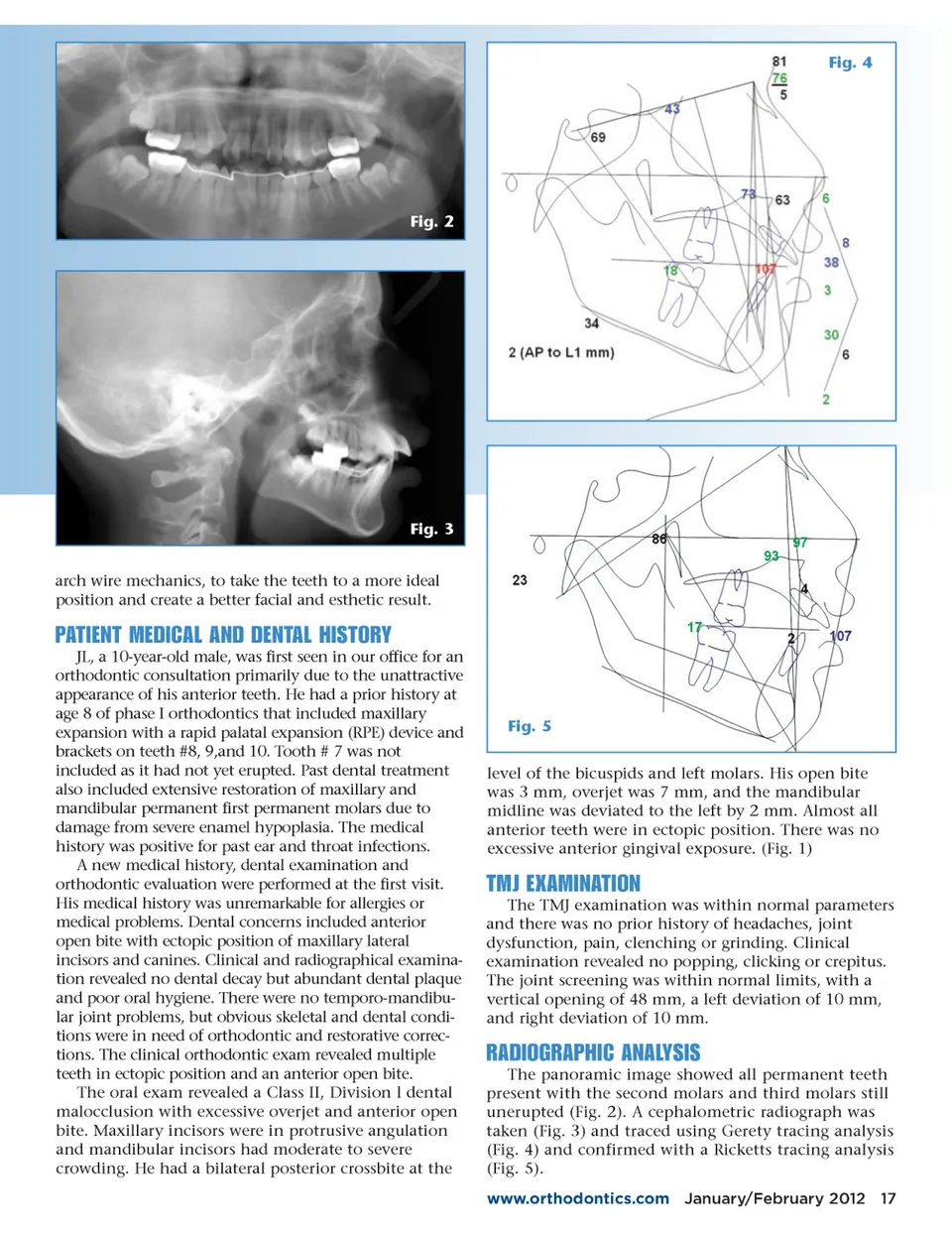
Fig. 4 Fig. 2 Fig. 3 arch wire mechanics, to take the teeth to a more ideal position and create a better facial and esthetic result. PATIENT MEDICAL AND DENTAL HISTORY JL, a 10-year-old male, was first seen in our office for an orthodontic consultation primarily due to the unattractive appearance of his anterior teeth. He had a prior history at age 8 of phase I orthodontics that included maxillary expansion with a rapid palatal expansion (RPE) device and brackets on teeth #8, 9,and 10. Tooth # 7 was not included as it had not yet erupted. Past dental treatment also included extensive restoration of maxillary and mandibular permanent first permanent molars due to damage from severe enamel hypoplasia. The medical history was positive for past ear and throat infections. A new medical history, dental examination and orthodontic evaluation were performed at the first visit. His medical history was unremarkable for allergies or medical problems. Dental concerns included anterior open bite with ectopic position of maxillary lateral incisors and canines. Clinical and radiographical examina-tion revealed no dental decay but abundant dental plaque and poor oral hygiene. There were no temporo-mandibu-lar joint problems, but obvious skeletal and dental condi-tions were in need of orthodontic and restorative correc-tions. The clinical orthodontic exam revealed multiple teeth in ectopic position and an anterior open bite. The oral exam revealed a Class II, Division l dental malocclusion with excessive overjet and anterior open bite. Maxillary incisors were in protrusive angulation and mandibular incisors had moderate to severe crowding. He had a bilateral posterior crossbite at the Fig. 5 level of the bicuspids and left molars. His open bite was 3 mm, overjet was 7 mm, and the mandibular midline was deviated to the left by 2 mm. Almost all anterior teeth were in ectopic position. There was no excessive anterior gingival exposure. (Fig. 1) TMJ EXAMINATION The TMJ examination was within normal parameters and there was no prior history of headaches, joint dysfunction, pain, clenching or grinding. Clinical examination revealed no popping, clicking or crepitus. The joint screening was within normal limits, with a vertical opening of 48 mm, a left deviation of 10 mm, and right deviation of 10 mm. RADIOGRAPHIC ANALYSIS The panoramic image showed all permanent teeth present with the second molars and third molars still unerupted (Fig. 2). A cephalometric radiograph was taken (Fig. 3) and traced using Gerety tracing analysis (Fig. 4) and confirmed with a Ricketts tracing analysis (Fig. 5). www.orthodontics.com January/February 2012 17
Journal of the American Orthodontic Society January-February 2012: Page 17