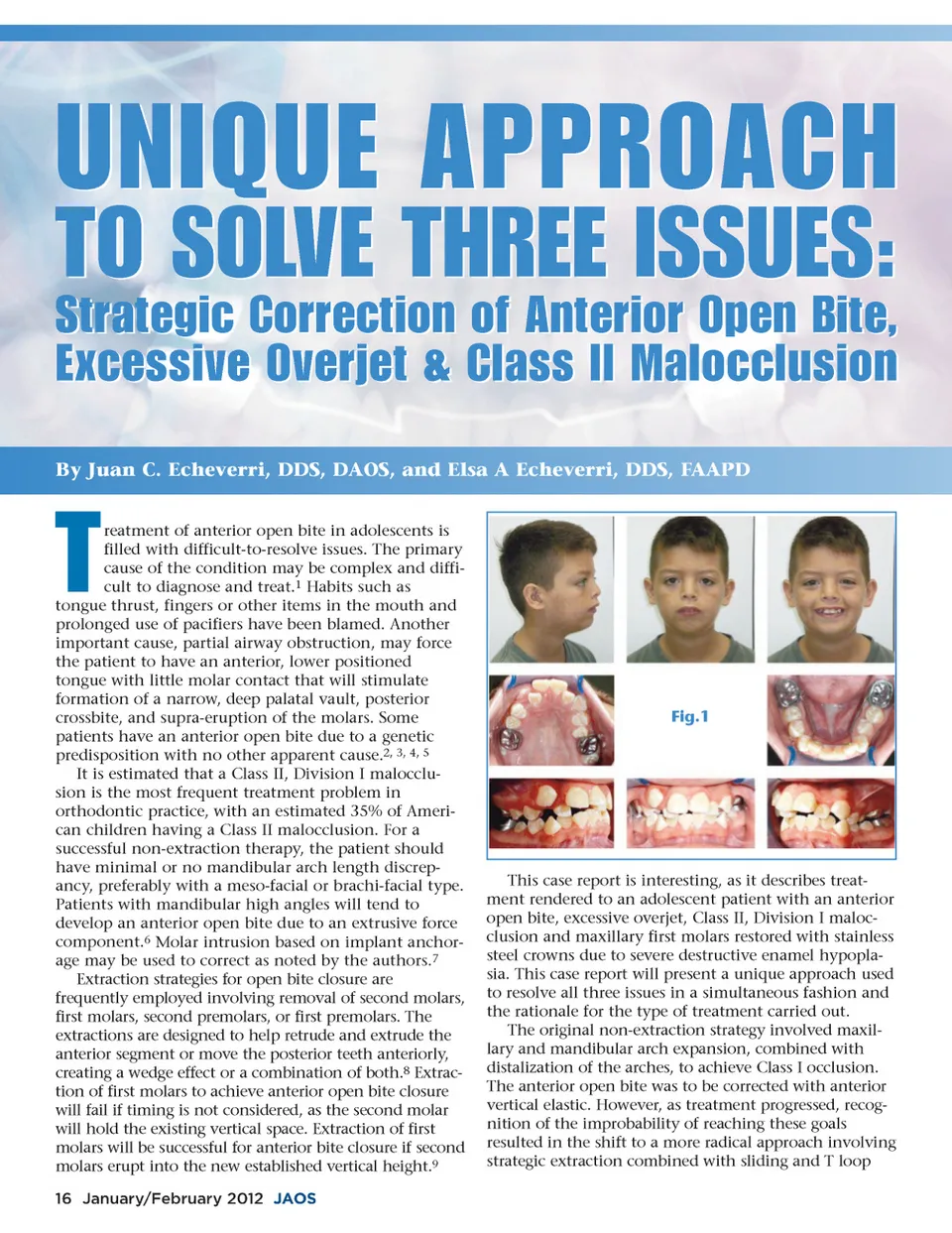
UNIQUE APPROACH TO SOLVE THREE ISSUES: Strategic Correction of Anterior Open Bite, Excessive Overjet & Class II Malocclusion By Juan C. Echeverri, DDS, DAOS, and Elsa A Echeverri, DDS, FAAPD T reatment of anterior open bite in adolescents is filled with difficult-to-resolve issues. The primary cause of the condition may be complex and diffi-cult to diagnose and treat. 1 Habits such as tongue thrust, fingers or other items in the mouth and prolonged use of pacifiers have been blamed. Another important cause, partial airway obstruction, may force the patient to have an anterior, lower positioned tongue with little molar contact that will stimulate formation of a narrow, deep palatal vault, posterior crossbite, and supra-eruption of the molars. Some patients have an anterior open bite due to a genetic predisposition with no other apparent cause. 2, 3, 4, 5 It is estimated that a Class II, Division I malocclu-sion is the most frequent treatment problem in orthodontic practice, with an estimated 35% of Ameri-can children having a Class II malocclusion. For a successful non-extraction therapy, the patient should have minimal or no mandibular arch length discrep-ancy, preferably with a meso-facial or brachi-facial type. Patients with mandibular high angles will tend to develop an anterior open bite due to an extrusive force component. 6 Molar intrusion based on implant anchor-age may be used to correct as noted by the authors. 7 Extraction strategies for open bite closure are frequently employed involving removal of second molars, first molars, second premolars, or first premolars. The extractions are designed to help retrude and extrude the anterior segment or move the posterior teeth anteriorly, creating a wedge effect or a combination of both. 8 Extrac-tion of first molars to achieve anterior open bite closure will fail if timing is not considered, as the second molar will hold the existing vertical space. Extraction of first molars will be successful for anterior bite closure if second molars erupt into the new established vertical height. 9 Fig.1 This case report is interesting, as it describes treat-ment rendered to an adolescent patient with an anterior open bite, excessive overjet, Class II, Division I maloc-clusion and maxillary first molars restored with stainless steel crowns due to severe destructive enamel hypopla-sia. This case report will present a unique approach used to resolve all three issues in a simultaneous fashion and the rationale for the type of treatment carried out. The original non-extraction strategy involved maxil-lary and mandibular arch expansion, combined with distalization of the arches, to achieve Class I occlusion. The anterior open bite was to be corrected with anterior vertical elastic. However, as treatment progressed, recog-nition of the improbability of reaching these goals resulted in the shift to a more radical approach involving strategic extraction combined with sliding and T loop 16 January/February 2012 JAOS
Journal of the American Orthodontic Society January-February 2012: Page 16