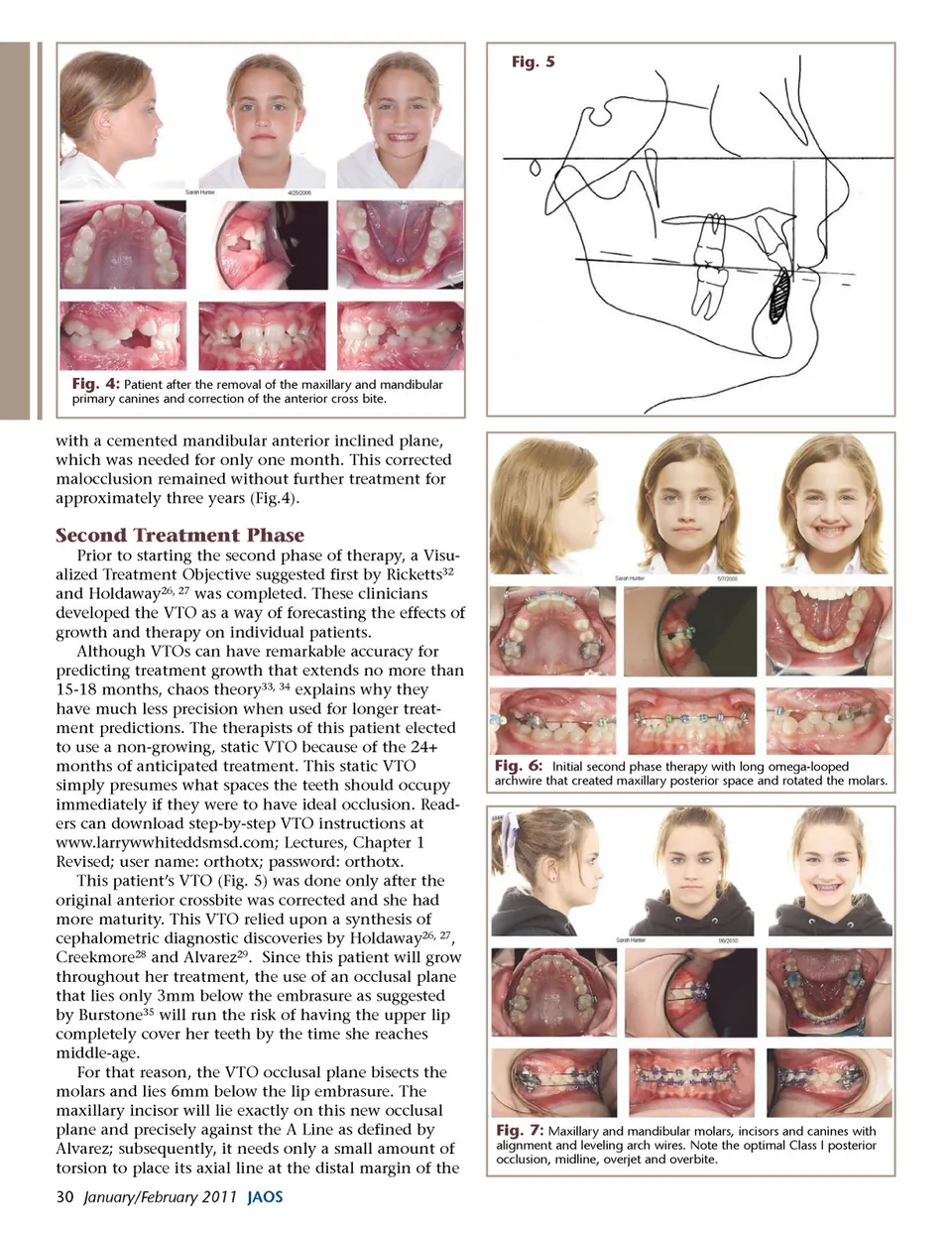
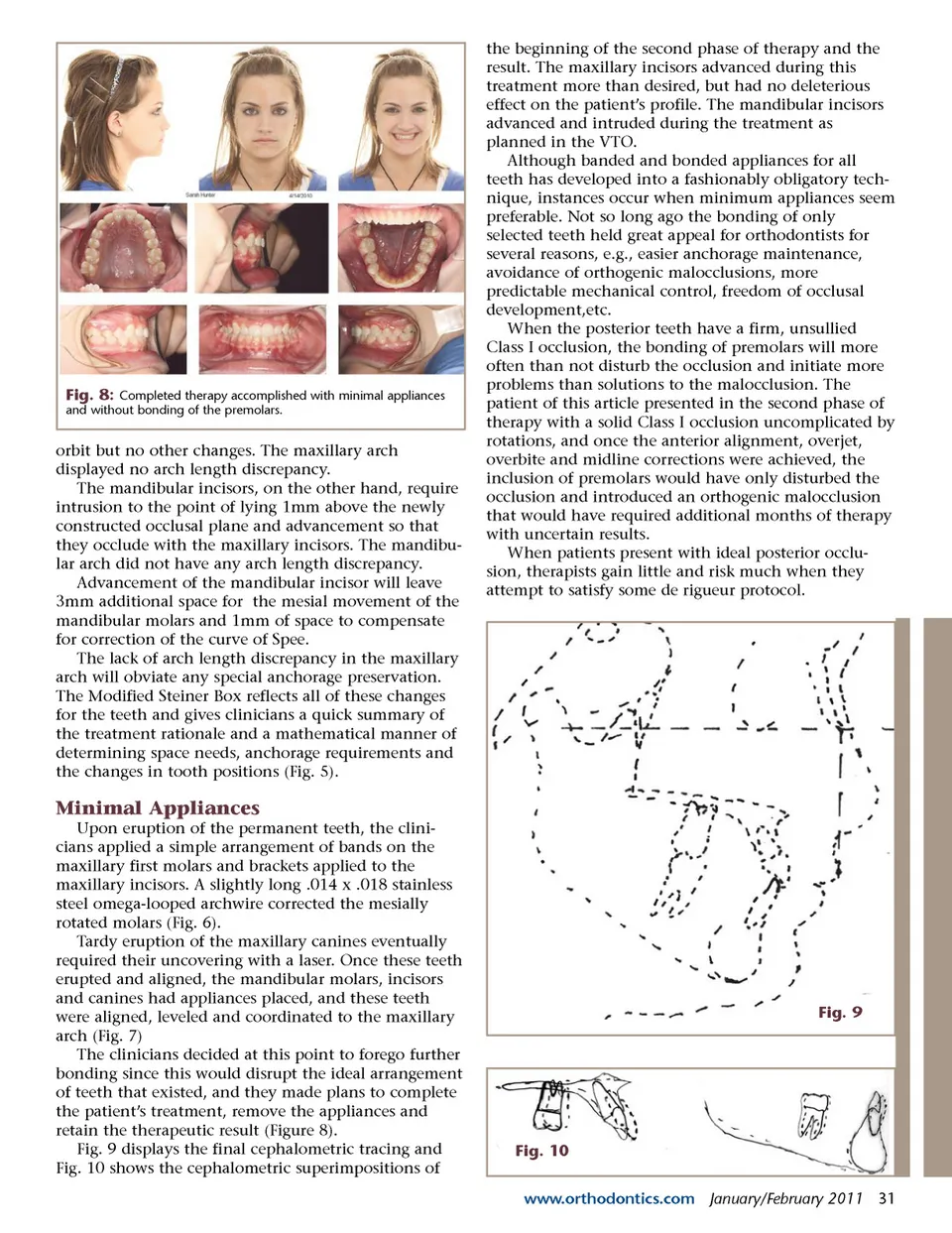
Fig. 5 Fig. 4: Patient after the removal of the maxillary and mandibular primary canines and correction of the anterior cross bite. with a cemented mandibular anterior inclined plane, which was needed for only one month. This corrected malocclusion remained without further treatment for approximately three years (Fig.4). Second Treatment Phase Prior to starting the second phase of therapy, a Visu-alized Treatment Objective suggested first by Ricketts 32 and Holdaway 26, 27 was completed. These clinicians developed the VTO as a way of forecasting the effects of growth and therapy on individual patients. Although VTOs can have remarkable accuracy for predicting treatment growth that extends no more than 15-18 months, chaos theory 33, 34 explains why they have much less precision when used for longer treat-ment predictions. The therapists of this patient elected to use a non-growing, static VTO because of the 24+ months of anticipated treatment. This static VTO simply presumes what spaces the teeth should occupy immediately if they were to have ideal occlusion. Read-ers can download step-by-step VTO instructions at www.larrywwhiteddsmsd.com; Lectures, Chapter 1 Revised; user name: orthotx; password: orthotx. This patient’s VTO (Fig. 5) was done only after the original anterior crossbite was corrected and she had more maturity. This VTO relied upon a synthesis of cephalometric diagnostic discoveries by Holdaway 26, 27 , Creekmore 28 and Alvarez 29 . Since this patient will grow throughout her treatment, the use of an occlusal plane that lies only 3mm below the embrasure as suggested by Burstone 35 will run the risk of having the upper lip completely cover her teeth by the time she reaches middle-age. For that reason, the VTO occlusal plane bisects the molars and lies 6mm below the lip embrasure. The maxillary incisor will lie exactly on this new occlusal plane and precisely against the A Line as defined by Alvarez; subsequently, it needs only a small amount of torsion to place its axial line at the distal margin of the 30 January/February 2011 JAOS Fig. 6: Initial second phase therapy with long omega-looped archwire that created maxillary posterior space and rotated the molars. Fig. 7: Maxillary and mandibular molars, incisors and canines with alignment and leveling arch wires. Note the optimal Class I posterior occlusion, midline, overjet and overbite.
Journal of the American Orthodontic Society January - February 2011: Page 30