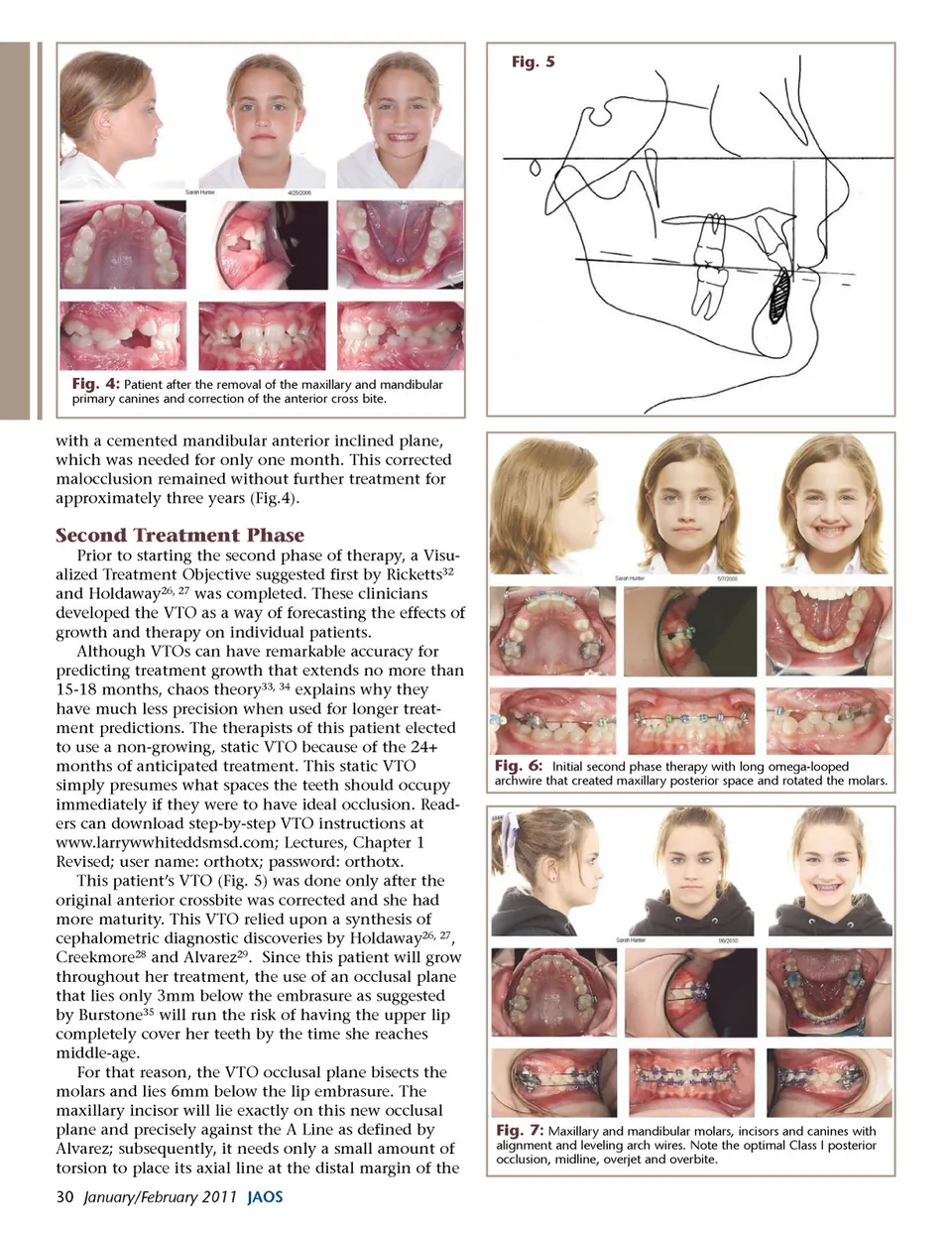
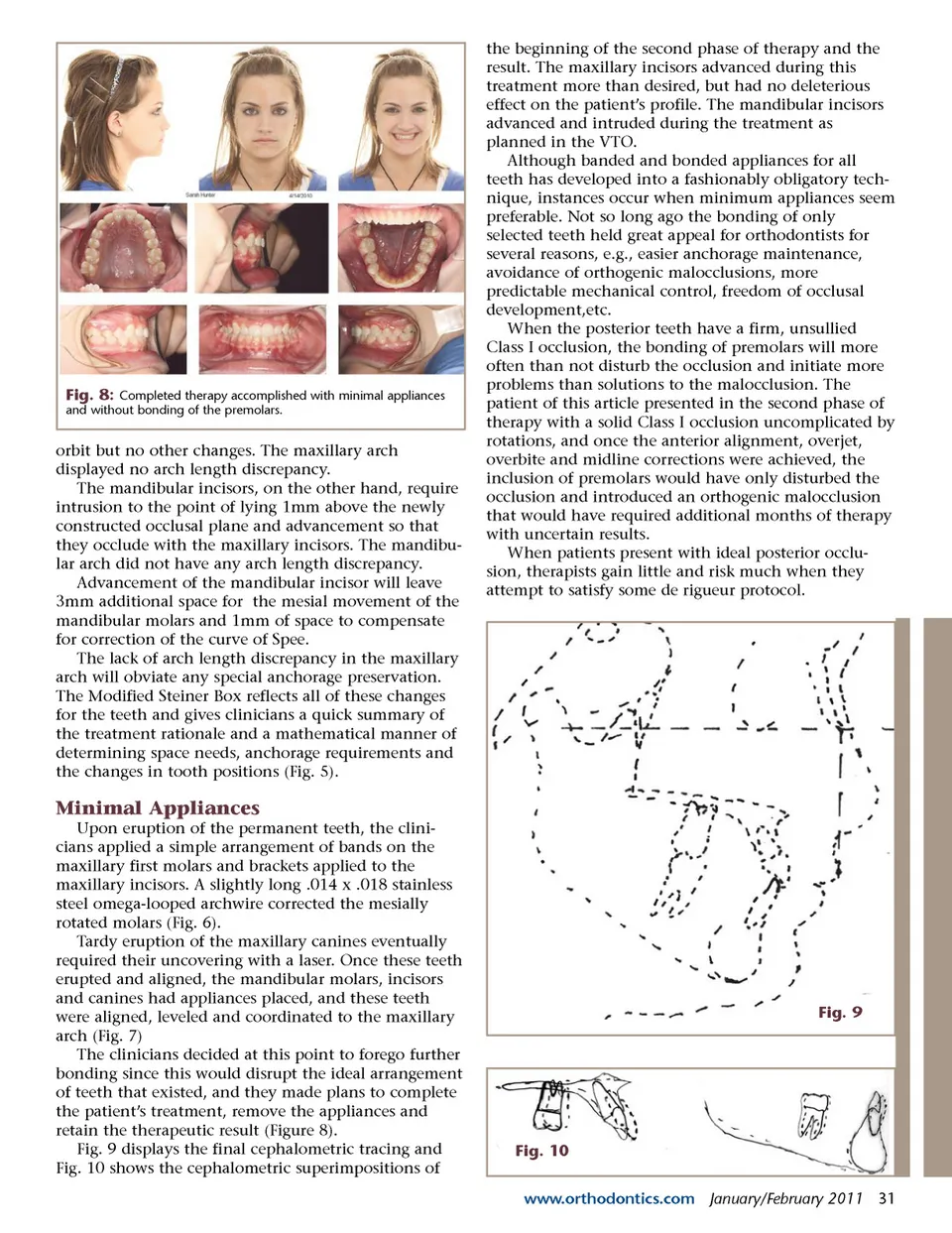
Fig. 8: Completed therapy accomplished with minimal appliances and without bonding of the premolars. orbit but no other changes. The maxillary arch displayed no arch length discrepancy. The mandibular incisors, on the other hand, require intrusion to the point of lying 1mm above the newly constructed occlusal plane and advancement so that they occlude with the maxillary incisors. The mandibu-lar arch did not have any arch length discrepancy. Advancement of the mandibular incisor will leave 3mm additional space for the mesial movement of the mandibular molars and 1mm of space to compensate for correction of the curve of Spee. The lack of arch length discrepancy in the maxillary arch will obviate any special anchorage preservation. The Modified Steiner Box reflects all of these changes for the teeth and gives clinicians a quick summary of the treatment rationale and a mathematical manner of determining space needs, anchorage requirements and the changes in tooth positions (Fig. 5). the beginning of the second phase of therapy and the result. The maxillary incisors advanced during this treatment more than desired, but had no deleterious effect on the patient’s profile. The mandibular incisors advanced and intruded during the treatment as planned in the VTO. Although banded and bonded appliances for all teeth has developed into a fashionably obligatory tech-nique, instances occur when minimum appliances seem preferable. Not so long ago the bonding of only selected teeth held great appeal for orthodontists for several reasons, e.g., easier anchorage maintenance, avoidance of orthogenic malocclusions, more predictable mechanical control, freedom of occlusal development,etc. When the posterior teeth have a firm, unsullied Class I occlusion, the bonding of premolars will more often than not disturb the occlusion and initiate more problems than solutions to the malocclusion. The patient of this article presented in the second phase of therapy with a solid Class I occlusion uncomplicated by rotations, and once the anterior alignment, overjet, overbite and midline corrections were achieved, the inclusion of premolars would have only disturbed the occlusion and introduced an orthogenic malocclusion that would have required additional months of therapy with uncertain results. When patients present with ideal posterior occlu-sion, therapists gain little and risk much when they attempt to satisfy some de rigueur protocol. Minimal Appliances Upon eruption of the permanent teeth, the clini-cians applied a simple arrangement of bands on the maxillary first molars and brackets applied to the maxillary incisors. A slightly long .014 x .018 stainless steel omega-looped archwire corrected the mesially rotated molars (Fig. 6). Tardy eruption of the maxillary canines eventually required their uncovering with a laser. Once these teeth erupted and aligned, the mandibular molars, incisors and canines had appliances placed, and these teeth were aligned, leveled and coordinated to the maxillary arch (Fig. 7) The clinicians decided at this point to forego further bonding since this would disrupt the ideal arrangement of teeth that existed, and they made plans to complete the patient’s treatment, remove the appliances and retain the therapeutic result (Figure 8). Fig. 9 displays the final cephalometric tracing and Fig. 10 shows the cephalometric superimpositions of Fig. 9 Fig. 10 www.orthodontics.com January/February 2011 31
Journal of the American Orthodontic Society January - February 2011: Page 31