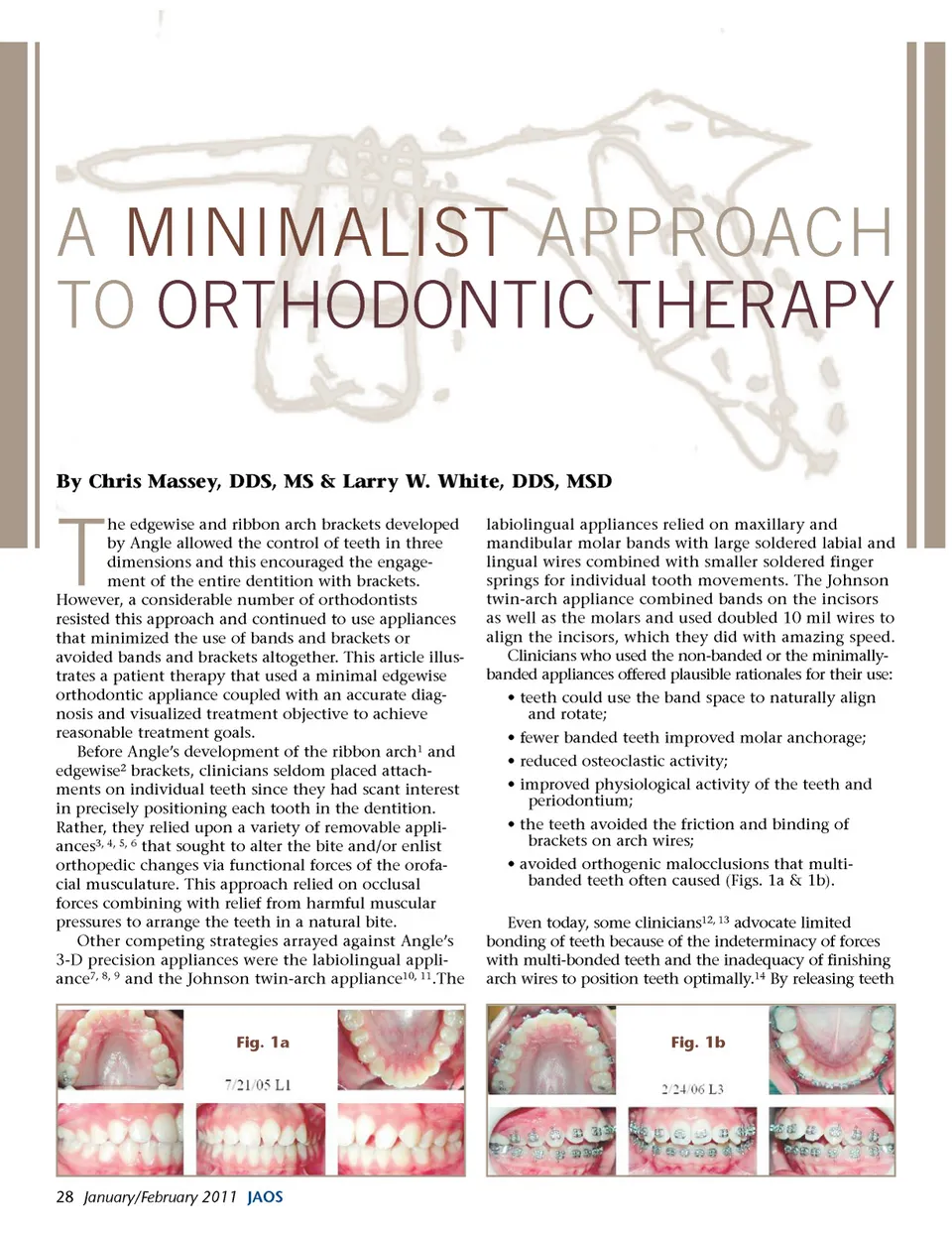
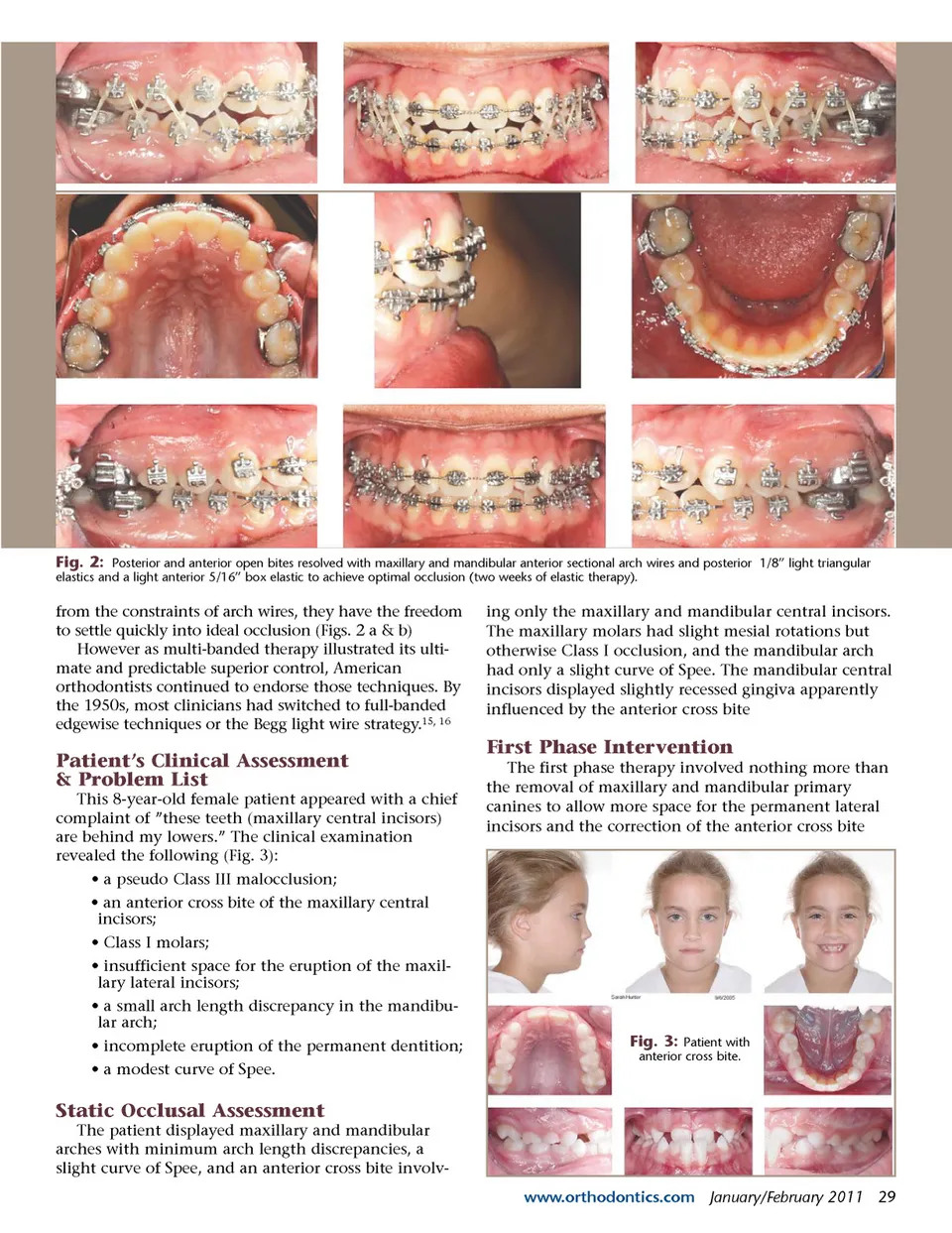
Fig. 2: Posterior and anterior open bites resolved with maxillary and mandibular anterior sectional arch wires and posterior 1/8” light triangular elastics and a light anterior 5/16” box elastic to achieve optimal occlusion (two weeks of elastic therapy). from the constraints of arch wires, they have the freedom to settle quickly into ideal occlusion (Figs. 2 a & b) However as multi-banded therapy illustrated its ulti-mate and predictable superior control, American orthodontists continued to endorse those techniques. By the 1950s, most clinicians had switched to full-banded edgewise techniques or the Begg light wire strategy. 15, 16 ing only the maxillary and mandibular central incisors. The maxillary molars had slight mesial rotations but otherwise Class I occlusion, and the mandibular arch had only a slight curve of Spee. The mandibular central incisors displayed slightly recessed gingiva apparently influenced by the anterior cross bite Patient’s Clinical Assessment & Problem List This 8-year-old female patient appeared with a chief complaint of ”these teeth (maxillary central incisors) are behind my lowers.” The clinical examination revealed the following (Fig. 3): • a pseudo Class III malocclusion; • an anterior cross bite of the maxillary central incisors; • Class I molars; • insufficient space for the eruption of the maxil-lary lateral incisors; • a small arch length discrepancy in the mandibu-lar arch; • incomplete eruption of the permanent dentition; • a modest curve of Spee. First Phase Intervention The first phase therapy involved nothing more than the removal of maxillary and mandibular primary canines to allow more space for the permanent lateral incisors and the correction of the anterior cross bite Fig. 3: Patient with anterior cross bite. Static Occlusal Assessment The patient displayed maxillary and mandibular arches with minimum arch length discrepancies, a slight curve of Spee, and an anterior cross bite involv-www.orthodontics.com January/February 2011 29
Journal of the American Orthodontic Society January - February 2011: Page 29