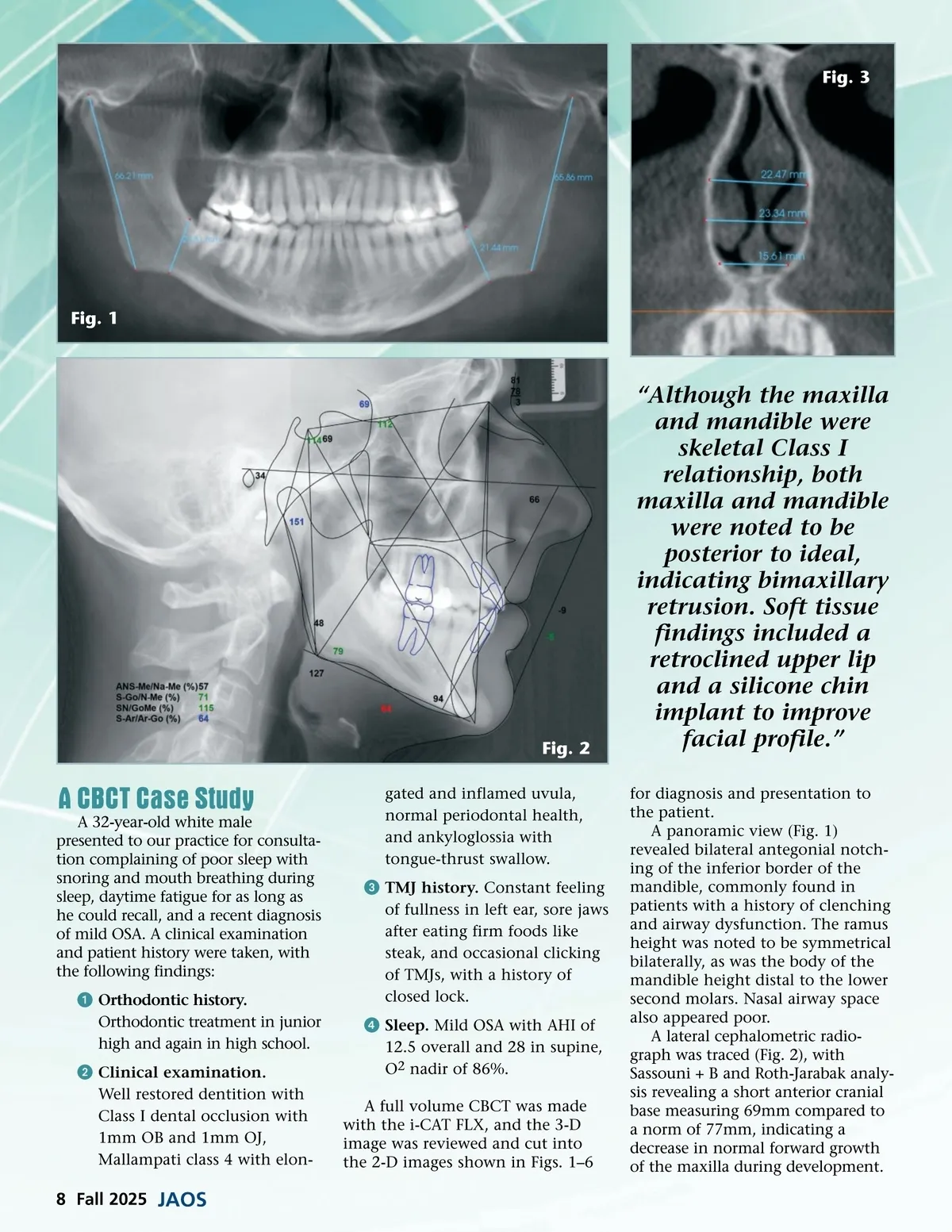
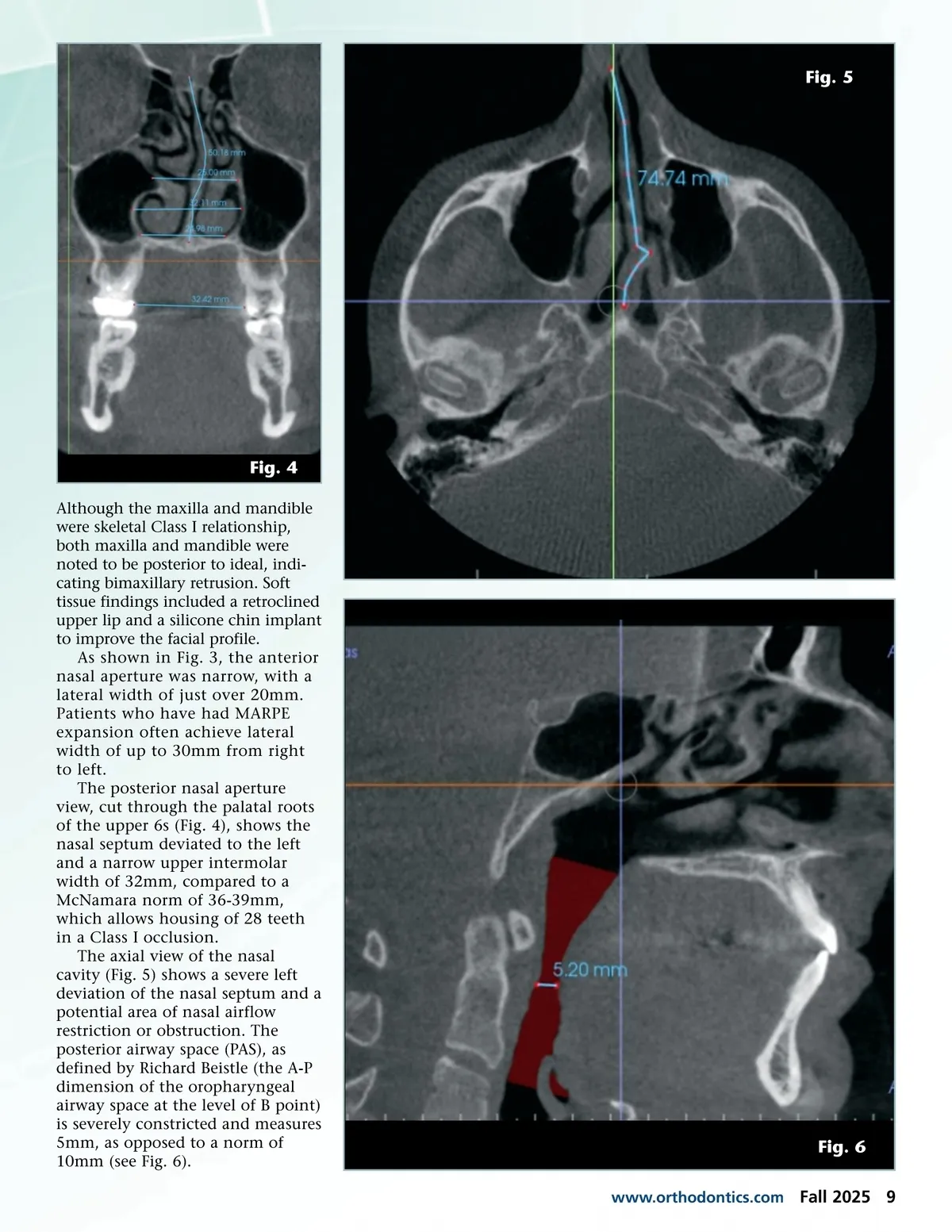
Fig. 5 Fig. 4 Although the maxilla and mandible were skeletal Class I relationship, both maxilla and mandible were noted to be posterior to ideal, indi-cating bimaxillary retrusion. Soft tissue findings included a retroclined upper lip and a silicone chin implant to improve the facial profile. As shown in Fig. 3, the anterior nasal aperture was narrow, with a lateral width of just over 20mm. Patients who have had MARPE expansion often achieve lateral width of up to 30mm from right to left. The posterior nasal aperture view, cut through the palatal roots of the upper 6s (Fig. 4), shows the nasal septum deviated to the left and a narrow upper intermolar width of 32mm, compared to a McNamara norm of 36-39mm, which allows housing of 28 teeth in a Class I occlusion. The axial view of the nasal cavity (Fig. 5) shows a severe left deviation of the nasal septum and a potential area of nasal airflow restriction or obstruction. The posterior airway space (PAS), as defined by Richard Beistle (the A-P dimension of the oropharyngeal airway space at the level of B point) is severely constricted and measures 5mm, as opposed to a norm of 10mm (see Fig. 6). www.orthodontics.com Fig. 6 Fall 2025 9
Journal of the American Orthodontic Society Fall 2025: Page 9