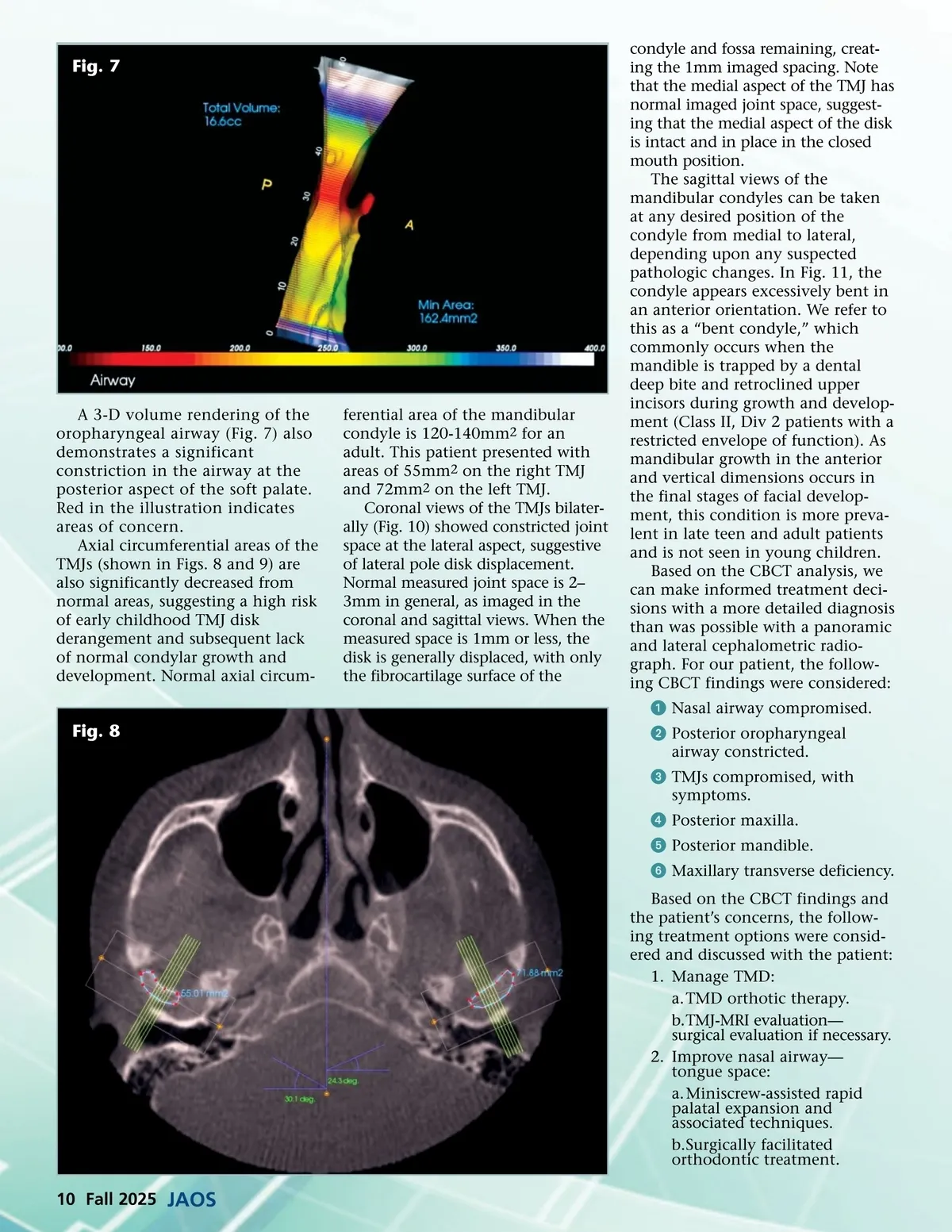
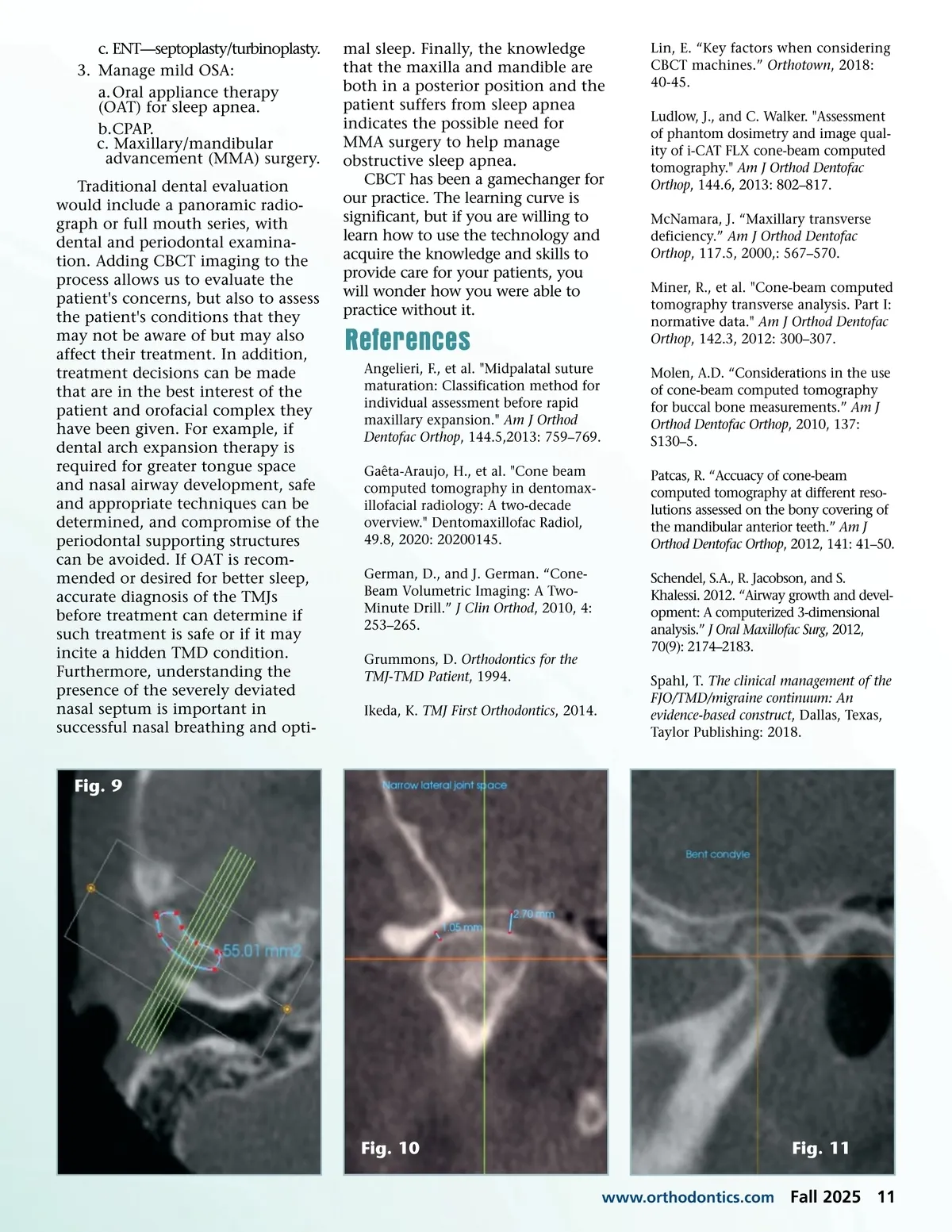
Fig. 7 A 3-D volume rendering of the oropharyngeal airway (Fig. 7) also demonstrates a significant constriction in the airway at the posterior aspect of the soft palate. Red in the illustration indicates areas of concern. Axial circumferential areas of the TMJs (shown in Figs. 8 and 9) are also significantly decreased from normal areas, suggesting a high risk of early childhood TMJ disk derangement and subsequent lack of normal condylar growth and development. Normal axial circum-ferential area of the mandibular condyle is 120-140mm 2 for an adult. This patient presented with areas of 55mm 2 on the right TMJ and 72mm 2 on the left TMJ. Coronal views of the TMJs bilater-ally (Fig. 10) showed constricted joint space at the lateral aspect, suggestive of lateral pole disk displacement. Normal measured joint space is 2– 3mm in general, as imaged in the coronal and sagittal views. When the measured space is 1mm or less, the disk is generally displaced, with only the fibrocartilage surface of the condyle and fossa remaining, creat-ing the 1mm imaged spacing. Note that the medial aspect of the TMJ has normal imaged joint space, suggest-ing that the medial aspect of the disk is intact and in place in the closed mouth position. The sagittal views of the mandibular condyles can be taken at any desired position of the condyle from medial to lateral, depending upon any suspected pathologic changes. In Fig. 11, the condyle appears excessively bent in an anterior orientation. We refer to this as a “bent condyle,” which commonly occurs when the mandible is trapped by a dental deep bite and retroclined upper incisors during growth and develop-ment (Class II, Div 2 patients with a restricted envelope of function). As mandibular growth in the anterior and vertical dimensions occurs in the final stages of facial develop-ment, this condition is more preva-lent in late teen and adult patients and is not seen in young children. Based on the CBCT analysis, we can make informed treatment deci-sions with a more detailed diagnosis than was possible with a panoramic and lateral cephalometric radio-graph. For our patient, the follow-ing CBCT findings were considered: ᕡ Nasal airway compromised. ᕢ Posterior oropharyngeal airway constricted. ᕣ TMJs compromised, with symptoms. ᕤ Posterior maxilla. ᕥ Posterior mandible. ᕦ Maxillary transverse deficiency. Based on the CBCT findings and the patient’s concerns, the follow-ing treatment options were consid-ered and discussed with the patient: 1. Manage TMD: a. TMD orthotic therapy. b.TMJ-MRI evaluation— surgical evaluation if necessary. 2. Improve nasal airway— tongue space: a. Miniscrew-assisted rapid palatal expansion and associated techniques. b.Surgically facilitated orthodontic treatment. Fig. 8 10 Fall 2025 JAOS
Journal of the American Orthodontic Society Fall 2025: Page 10