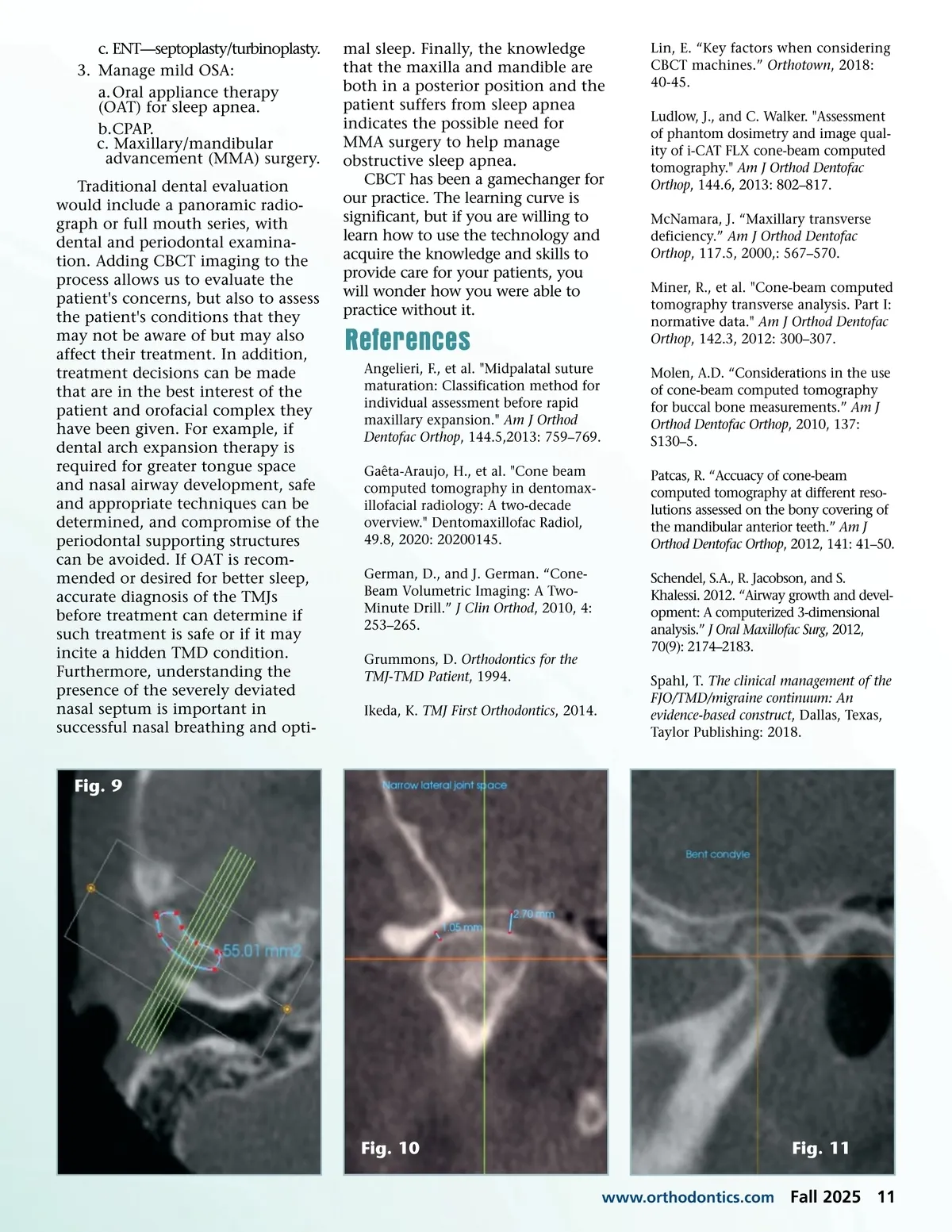
c. ENT—septoplasty/turbinoplasty. 3. Manage mild OSA: a. Oral appliance therapy (OAT) for sleep apnea. b.CPAP. c. Maxillary/mandibular advancement (MMA) surgery. Traditional dental evaluation would include a panoramic radio-graph or full mouth series, with dental and periodontal examina-tion. Adding CBCT imaging to the process allows us to evaluate the patient's concerns, but also to assess the patient's conditions that they may not be aware of but may also affect their treatment. In addition, treatment decisions can be made that are in the best interest of the patient and orofacial complex they have been given. For example, if dental arch expansion therapy is required for greater tongue space and nasal airway development, safe and appropriate techniques can be determined, and compromise of the periodontal supporting structures can be avoided. If OAT is recom-mended or desired for better sleep, accurate diagnosis of the TMJs before treatment can determine if such treatment is safe or if it may incite a hidden TMD condition. Furthermore, understanding the presence of the severely deviated nasal septum is important in successful nasal breathing and opti-mal sleep. Finally, the knowledge that the maxilla and mandible are both in a posterior position and the patient suffers from sleep apnea indicates the possible need for MMA surgery to help manage obstructive sleep apnea. CBCT has been a gamechanger for our practice. The learning curve is significant, but if you are willing to learn how to use the technology and acquire the knowledge and skills to provide care for your patients, you will wonder how you were able to practice without it. Lin, E. “Key factors when considering CBCT machines.” Orthotown , 2018: 40-45. Ludlow, J., and C. Walker. "Assessment of phantom dosimetry and image qual-ity of i-CAT FLX cone-beam computed tomography." Am J Orthod Dentofac Orthop , 144.6, 2013: 802–817. McNamara, J. “Maxillary transverse deficiency.” Am J Orthod Dentofac Orthop , 117.5, 2000,: 567–570. Miner, R., et al. "Cone-beam computed tomography transverse analysis. Part I: normative data." Am J Orthod Dentofac Orthop , 142.3, 2012: 300–307. Molen, A.D. “Considerations in the use of cone-beam computed tomography for buccal bone measurements.” Am J Orthod Dentofac Orthop , 2010, 137: S130–5. Patcas, R. “Accuacy of cone-beam computed tomography at different reso-lutions assessed on the bony covering of the mandibular anterior teeth.” Am J Orthod Dentofac Orthop , 2012, 141: 41–50. Schendel, S.A., R. Jacobson, and S. Khalessi. 2012. “Airway growth and devel-opment: A computerized 3-dimensional analysis.” J Oral Maxillofac Surg , 2012, 70(9): 2174–2183. Spahl, T. The clinical management of the FJO/TMD/migraine continuum: An evidence-based construct , Dallas, Texas, Taylor Publishing: 2018. References Angelieri, F., et al. "Midpalatal suture maturation: Classification method for individual assessment before rapid maxillary expansion." Am J Orthod Dentofac Orthop , 144.5,2013: 759–769. Gaêta-Araujo, H., et al. "Cone beam computed tomography in dentomax-illofacial radiology: A two-decade overview." Dentomaxillofac Radiol, 49.8, 2020: 20200145. German, D., and J. German. “Cone-Beam Volumetric Imaging: A Two-Minute Drill.” J Clin Orthod , 2010, 4: 253–265. Grummons, D. Orthodontics for the TMJ-TMD Patient , 1994. Ikeda, K. TMJ First Orthodontics , 2014. Fig. 9 Fig. 10 www.orthodontics.com Fig. 11 Fall 2025 11
Journal of the American Orthodontic Society Fall 2025: Page 11