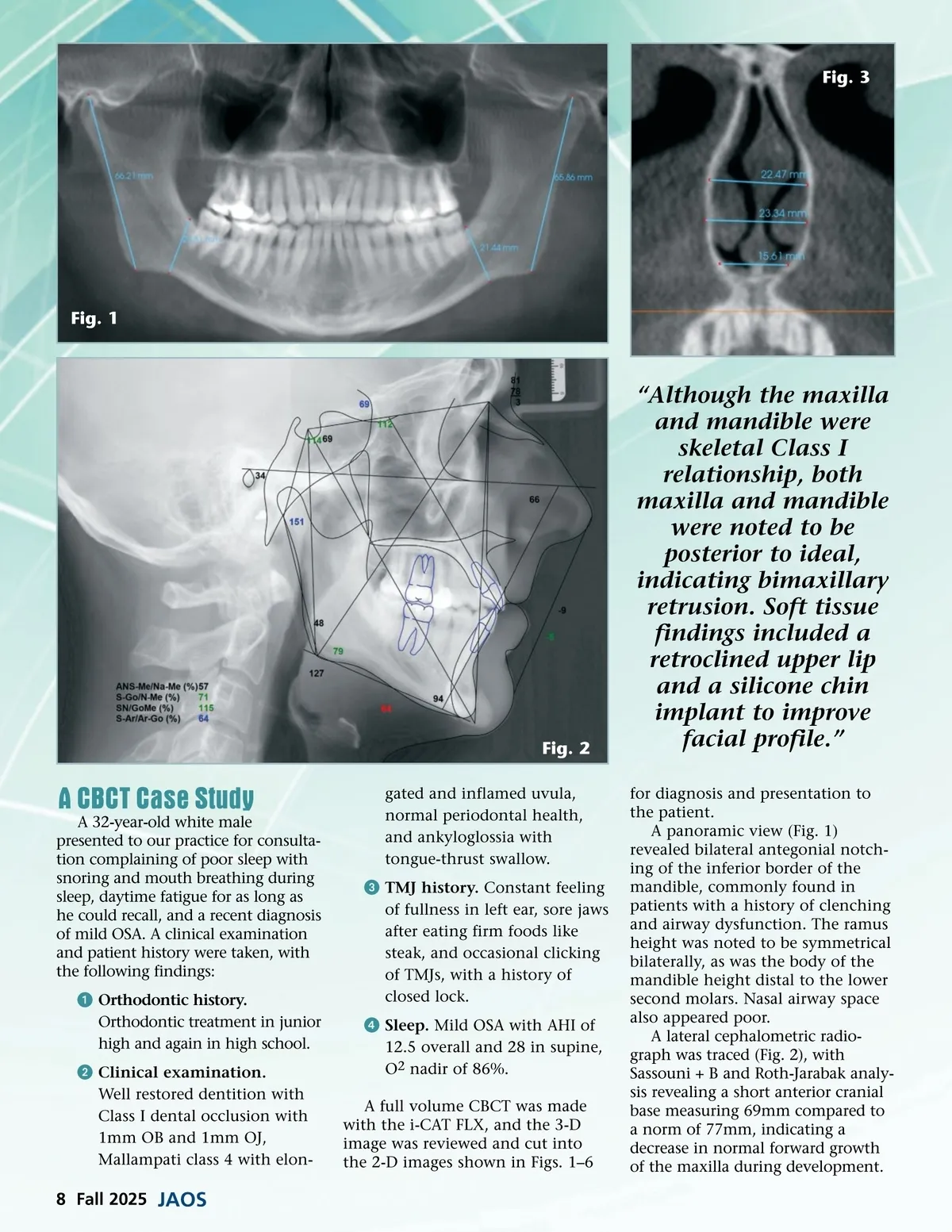
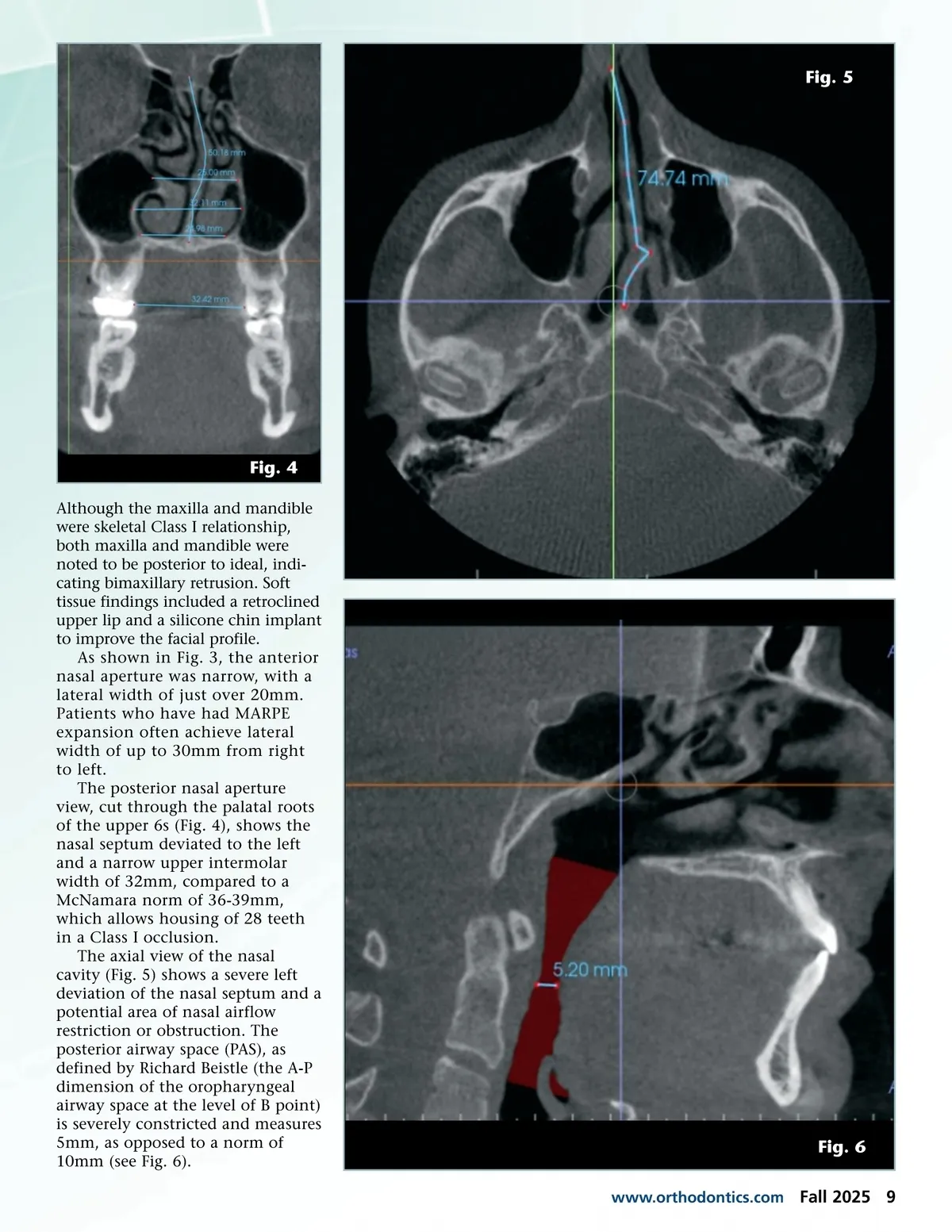
Fig. 3 Fig. 1 Fig. 2 “Although the maxilla and mandible were skeletal Class I relationship, both maxilla and mandible were noted to be posterior to ideal, indicating bimaxillary retrusion. Soft tissue findings included a retroclined upper lip and a silicone chin implant to improve facial profile.” for diagnosis and presentation to the patient. A panoramic view (Fig. 1) revealed bilateral antegonial notch-ing of the inferior border of the mandible, commonly found in patients with a history of clenching and airway dysfunction. The ramus height was noted to be symmetrical bilaterally, as was the body of the mandible height distal to the lower second molars. Nasal airway space also appeared poor. A lateral cephalometric radio-graph was traced (Fig. 2), with Sassouni + B and Roth-Jarabak analy-sis revealing a short anterior cranial base measuring 69mm compared to a norm of 77mm, indicating a decrease in normal forward growth of the maxilla during development. A CBCT Case Study A 32-year-old white male presented to our practice for consulta-tion complaining of poor sleep with snoring and mouth breathing during sleep, daytime fatigue for as long as he could recall, and a recent diagnosis of mild OSA. A clinical examination and patient history were taken, with the following findings: ᕡ Orthodontic history. Orthodontic treatment in junior high and again in high school. ᕢ Clinical examination. Well restored dentition with Class I dental occlusion with 1mm OB and 1mm OJ, Mallampati class 4 with elon-gated and inflamed uvula, normal periodontal health, and ankyloglossia with tongue-thrust swallow. ᕣ TMJ history. Constant feeling of fullness in left ear, sore jaws after eating firm foods like steak, and occasional clicking of TMJs, with a history of closed lock. ᕤ Sleep. Mild OSA with AHI of 12.5 overall and 28 in supine, O 2 nadir of 86%. A full volume CBCT was made with the i-CAT FLX, and the 3-D image was reviewed and cut into the 2-D images shown in Figs. 1–6 8 Fall 2025 JAOS
Journal of the American Orthodontic Society Fall 2025: Page 8