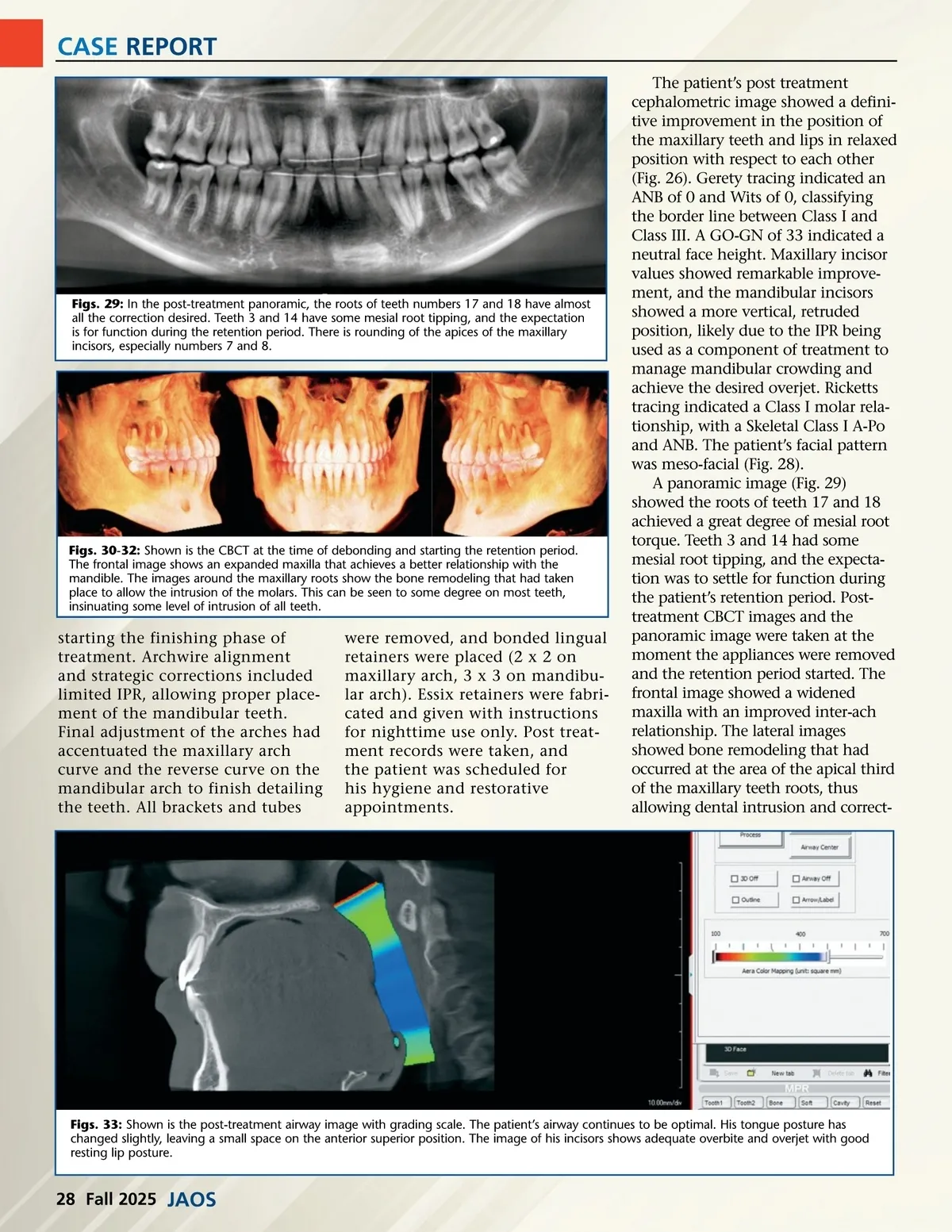
CASE REPORT Figs. 34: In the post-expansion axial image of the palatine suture, the suture borders appear diffuse compared to the pre-treatment suture image. This is most probably the effect of the expansion of this suture with the RPE. Figs. 35: The coronal image shows vertical alignment of the opposing molars. A crossbite relationship is avoided by proper expansion. All roots are within the dento-alveolar bone. ing the anterior open bite. This bone remodeling could be observed around the apex of most of the maxillary teeth, suggesting some intrusion at all levels of the arch (Figs 30–32). The post-treatment airway image included its grading scale. The airway was graded as optimum at time of imaging (Fig 21). The incisor relationship image was of adequate overbite and overjet with good resting lip posture (Fig. 33). The palatine suture after treatment was not as defined compared to its original shape before expansion (Fig. 18). This could be explained by expansion of the pala-tine suture that took place during treatment (Fig. 34) and the remodel-ing taking place in its new shape. The post-treatment coronal image showed vertical alignment of opposing molars. The roots were located under the crowns, with minimal buccal crown inclination. The crossbite relationship was avoided by proper expansion. All roots ended within the dento-alveolar bone (Fig. 35). The patient’s orthodontic case was challenging due his initial lack of commitment to appointments and behavior. His third round was successful, as he committed to all aspects required for a successful outcome. Key to the treatment planning was diagnosing the need for the molar intrusions to manage the anterior open bite, and the need and possibility to expand his maxillary arch based on the radiographic evidence. The patient and orthodontic team had a good rapport throughout treatment. In addition to the patient’s commit-ment, the successful outcome relied on proper diagnosis and implementation of an innovative combined expansion and intrusion design and traditional straight arch appliance techniques. The patient’s total active treat-ment time on the third round was 19 months. At the time of his final records, he had achieved a Class I dental relationship with adequate overjet and overbite. The patient’s face was balanced, with improved facial and dental aesthetics. He was pleased with the results, and all initial objectives were met (Fig. 25). The orthodontic therapy allowed challenging anatomical variations to be transformed, achieving a normal appearance for a young adult. References 1. Baumgaertel S, Smuthkochorn S, Palomo JM. Intrusion method for a single over-erupted maxillary molar using only palatal mini-implants and partial fixed appliances. AM J Orthod Dentofacial Orthop . 2016, 149(3), 411-5 2. Angelieri F, Cevidanes L, Franchi L , João R Gonçalves JR, E, McNamara JA Midpalatal suture maturation: Classifica-tion method for individual assessment before rapid maxillary expansion Am J Orthod Dentofacial Orthop . 2013 Nov;144(5):759–769 3. Echeverri JC, Echeverri E A: Anterior Open Bites: Appliance and technique helps improve mechanics of maxillary molar intrusion. JAOS 14, issue 3: 18 -24, 2014 4. Echeverri J C, Echeverri E A: Solving a dolichocephalic Class III Case with trans-verse constricted maxillary by using modified mechanical approaches. JAOS 20, issue 3: 14-20, 2020 5. Echeverri J C, Echeverri E A: Clinical case report: Management of Transverse Constriction Malocclusions in Adoles-cents. JAOS 23, issue 9: 16-25 2022 Figs. 36-37: A one-arm expansion screw by Dentaurum is used for fabrication of the expansion/ intrusion appliance and on the tomas-pin EP style head used to anchor to the palate for the intrusion force. www.orthodontics.com Fall 2025 29
Journal of the American Orthodontic Society Fall 2025: Page 29