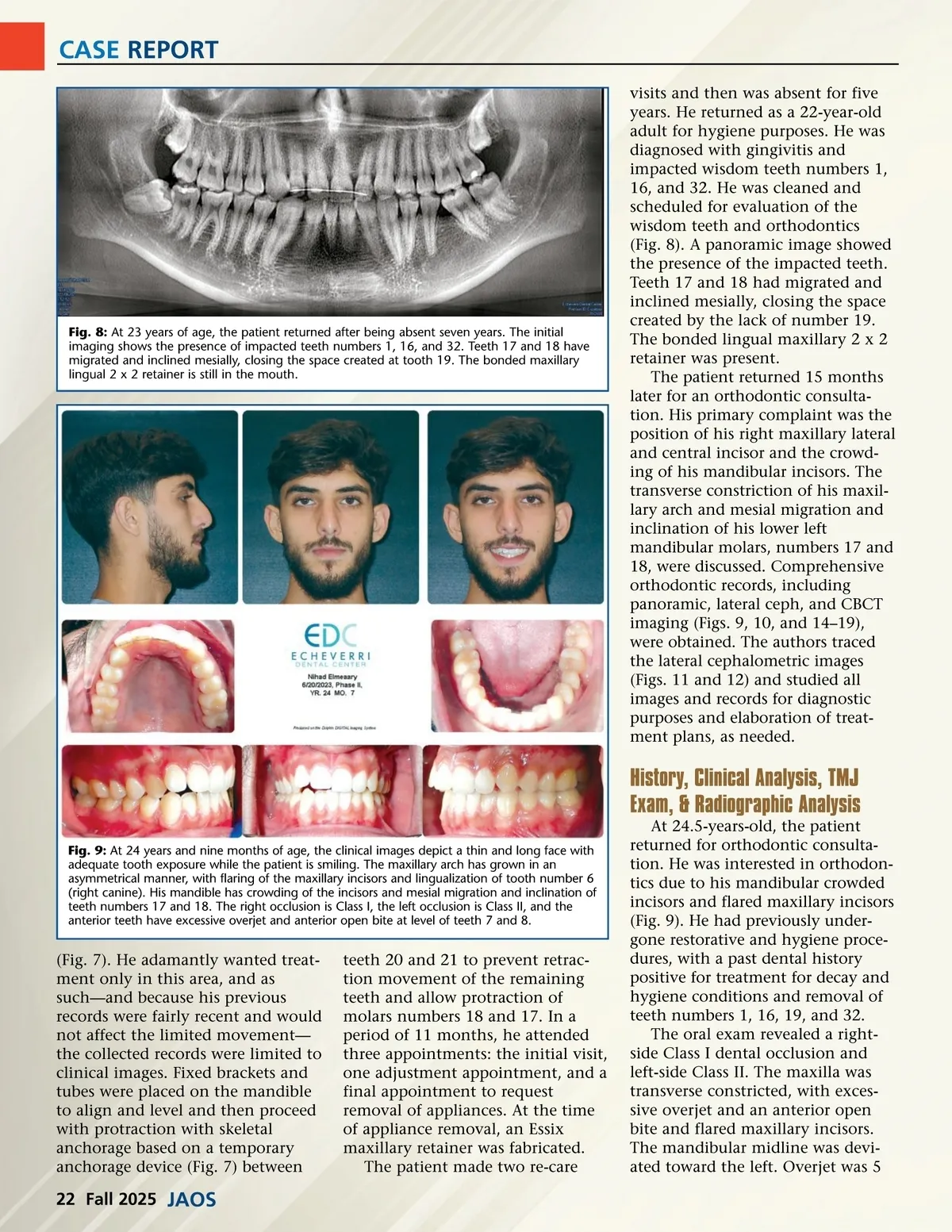
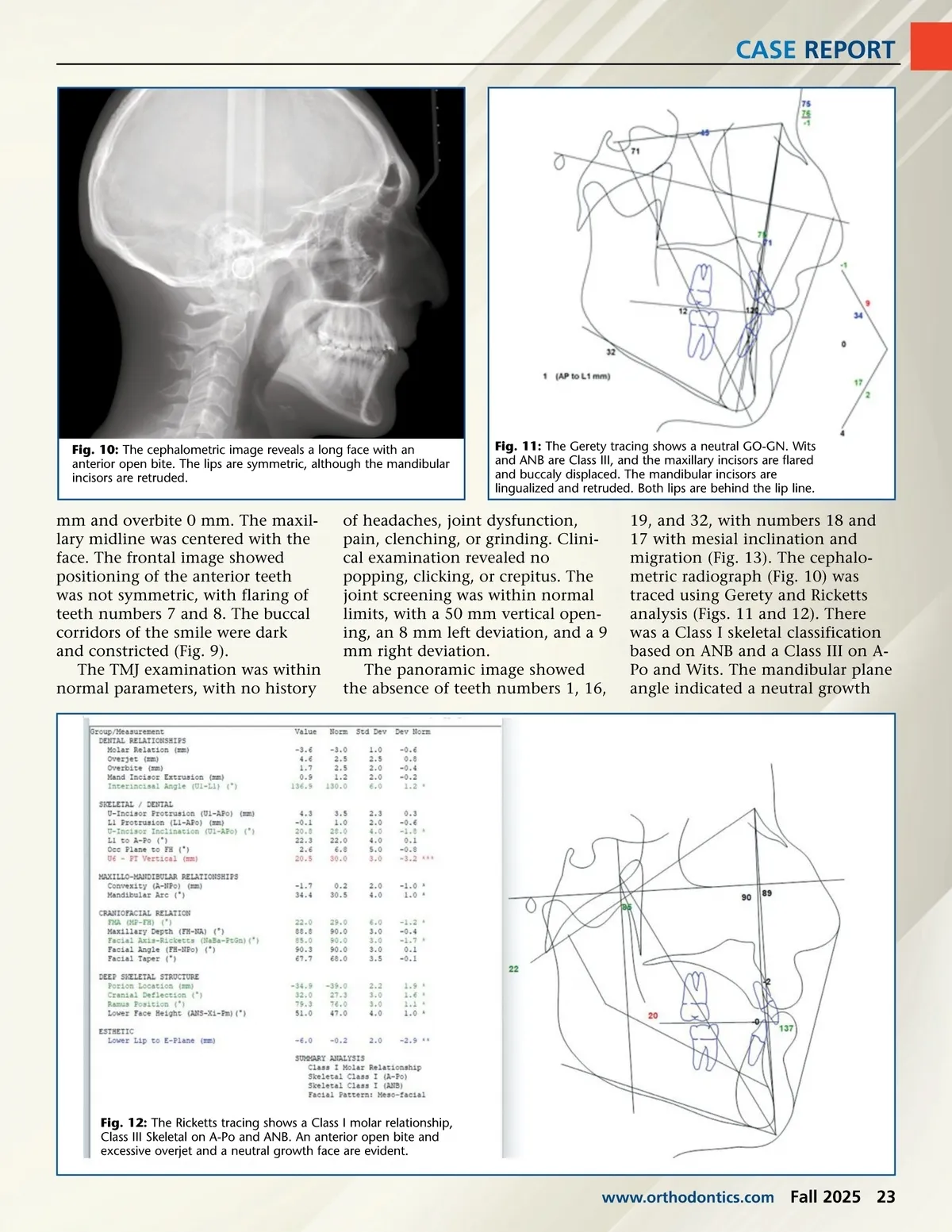
CASE REPORT visits and then was absent for five years. He returned as a 22-year-old adult for hygiene purposes. He was diagnosed with gingivitis and impacted wisdom teeth numbers 1, 16, and 32. He was cleaned and scheduled for evaluation of the wisdom teeth and orthodontics (Fig. 8). A panoramic image showed the presence of the impacted teeth. Teeth 17 and 18 had migrated and inclined mesially, closing the space created by the lack of number 19. The bonded lingual maxillary 2 x 2 retainer was present. The patient returned 15 months later for an orthodontic consulta-tion. His primary complaint was the position of his right maxillary lateral and central incisor and the crowd-ing of his mandibular incisors. The transverse constriction of his maxil-lary arch and mesial migration and inclination of his lower left mandibular molars, numbers 17 and 18, were discussed. Comprehensive orthodontic records, including panoramic, lateral ceph, and CBCT imaging (Figs. 9, 10, and 14–19), were obtained. The authors traced the lateral cephalometric images (Figs. 11 and 12) and studied all images and records for diagnostic purposes and elaboration of treat-ment plans, as needed. Fig. 8: At 23 years of age, the patient returned after being absent seven years. The initial imaging shows the presence of impacted teeth numbers 1, 16, and 32. Teeth 17 and 18 have migrated and inclined mesially, closing the space created at tooth 19. The bonded maxillary lingual 2 x 2 retainer is still in the mouth. History, Clinical Analysis, TMJ Exam, & Radiographic Analysis Fig. 9: At 24 years and nine months of age, the clinical images depict a thin and long face with adequate tooth exposure while the patient is smiling. The maxillary arch has grown in an asymmetrical manner, with flaring of the maxillary incisors and lingualization of tooth number 6 (right canine). His mandible has crowding of the incisors and mesial migration and inclination of teeth numbers 17 and 18. The right occlusion is Class I, the left occlusion is Class II, and the anterior teeth have excessive overjet and anterior open bite at level of teeth 7 and 8. (Fig. 7). He adamantly wanted treat-ment only in this area, and as such—and because his previous records were fairly recent and would not affect the limited movement— the collected records were limited to clinical images. Fixed brackets and tubes were placed on the mandible to align and level and then proceed with protraction with skeletal anchorage based on a temporary anchorage device (Fig. 7) between teeth 20 and 21 to prevent retrac-tion movement of the remaining teeth and allow protraction of molars numbers 18 and 17. In a period of 11 months, he attended three appointments: the initial visit, one adjustment appointment, and a final appointment to request removal of appliances. At the time of appliance removal, an Essix maxillary retainer was fabricated. The patient made two re-care At 24.5-years-old, the patient returned for orthodontic consulta-tion. He was interested in orthodon-tics due to his mandibular crowded incisors and flared maxillary incisors (Fig. 9). He had previously under-gone restorative and hygiene proce-dures, with a past dental history positive for treatment for decay and hygiene conditions and removal of teeth numbers 1, 16, 19, and 32. The oral exam revealed a right-side Class I dental occlusion and left-side Class II. The maxilla was transverse constricted, with exces-sive overjet and an anterior open bite and flared maxillary incisors. The mandibular midline was devi-ated toward the left. Overjet was 5 22 Fall 2025 JAOS
Journal of the American Orthodontic Society Fall 2025: Page 22