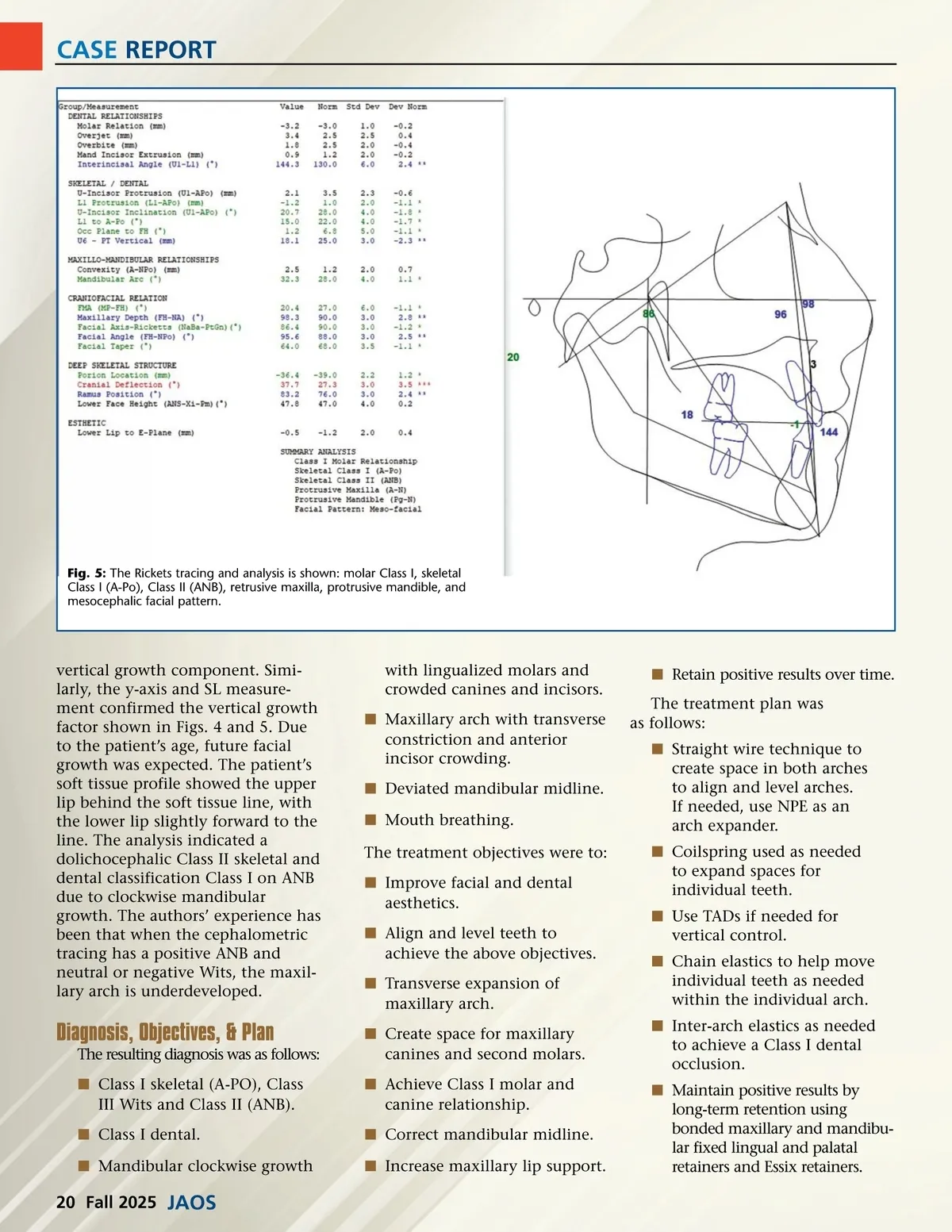
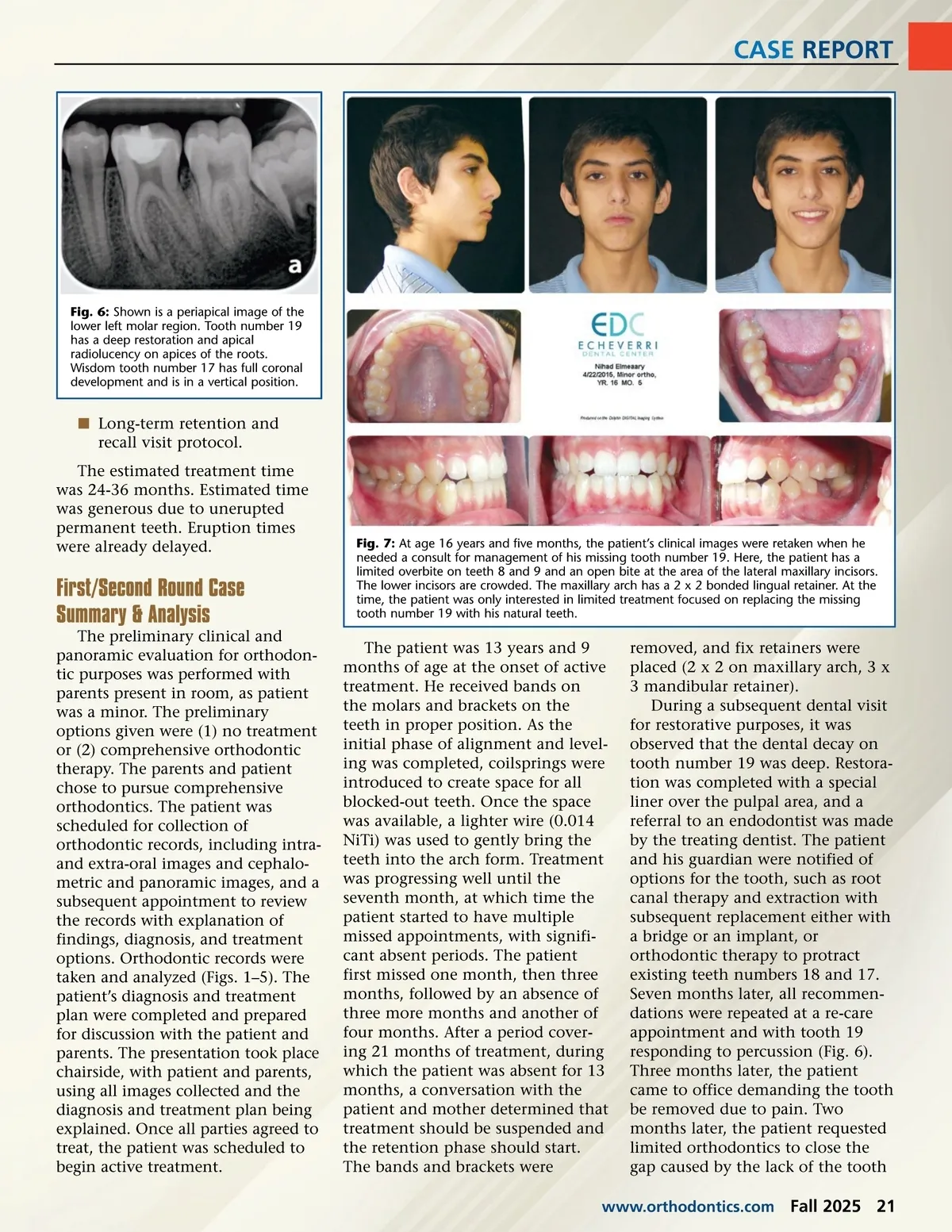
CASE REPORT Fig. 6: Shown is a periapical image of the lower left molar region. Tooth number 19 has a deep restoration and apical radiolucency on apices of the roots. Wisdom tooth number 17 has full coronal development and is in a vertical position. í Long-term retention and recall visit protocol. The estimated treatment time was 24-36 months. Estimated time was generous due to unerupted permanent teeth. Eruption times were already delayed. First/Second Round Case Summary & Analysis The preliminary clinical and panoramic evaluation for orthodon-tic purposes was performed with parents present in room, as patient was a minor. The preliminary options given were (1) no treatment or (2) comprehensive orthodontic therapy. The parents and patient chose to pursue comprehensive orthodontics. The patient was scheduled for collection of orthodontic records, including intra-and extra-oral images and cephalo-metric and panoramic images, and a subsequent appointment to review the records with explanation of findings, diagnosis, and treatment options. Orthodontic records were taken and analyzed (Figs. 1–5). The patient’s diagnosis and treatment plan were completed and prepared for discussion with the patient and parents. The presentation took place chairside, with patient and parents, using all images collected and the diagnosis and treatment plan being explained. Once all parties agreed to treat, the patient was scheduled to begin active treatment. Fig. 7: At age 16 years and five months, the patient’s clinical images were retaken when he needed a consult for management of his missing tooth number 19. Here, the patient has a limited overbite on teeth 8 and 9 and an open bite at the area of the lateral maxillary incisors. The lower incisors are crowded. The maxillary arch has a 2 x 2 bonded lingual retainer. At the time, the patient was only interested in limited treatment focused on replacing the missing tooth number 19 with his natural teeth. The patient was 13 years and 9 months of age at the onset of active treatment. He received bands on the molars and brackets on the teeth in proper position. As the initial phase of alignment and level-ing was completed, coilsprings were introduced to create space for all blocked-out teeth. Once the space was available, a lighter wire (0.014 NiTi) was used to gently bring the teeth into the arch form. Treatment was progressing well until the seventh month, at which time the patient started to have multiple missed appointments, with signifi-cant absent periods. The patient first missed one month, then three months, followed by an absence of three more months and another of four months. After a period cover-ing 21 months of treatment, during which the patient was absent for 13 months, a conversation with the patient and mother determined that treatment should be suspended and the retention phase should start. The bands and brackets were removed, and fix retainers were placed (2 x 2 on maxillary arch, 3 x 3 mandibular retainer). During a subsequent dental visit for restorative purposes, it was observed that the dental decay on tooth number 19 was deep. Restora-tion was completed with a special liner over the pulpal area, and a referral to an endodontist was made by the treating dentist. The patient and his guardian were notified of options for the tooth, such as root canal therapy and extraction with subsequent replacement either with a bridge or an implant, or orthodontic therapy to protract existing teeth numbers 18 and 17. Seven months later, all recommen-dations were repeated at a re-care appointment and with tooth 19 responding to percussion (Fig. 6). Three months later, the patient came to office demanding the tooth be removed due to pain. Two months later, the patient requested limited orthodontics to close the gap caused by the lack of the tooth www.orthodontics.com Fall 2025 21
Journal of the American Orthodontic Society Fall 2025: Page 21