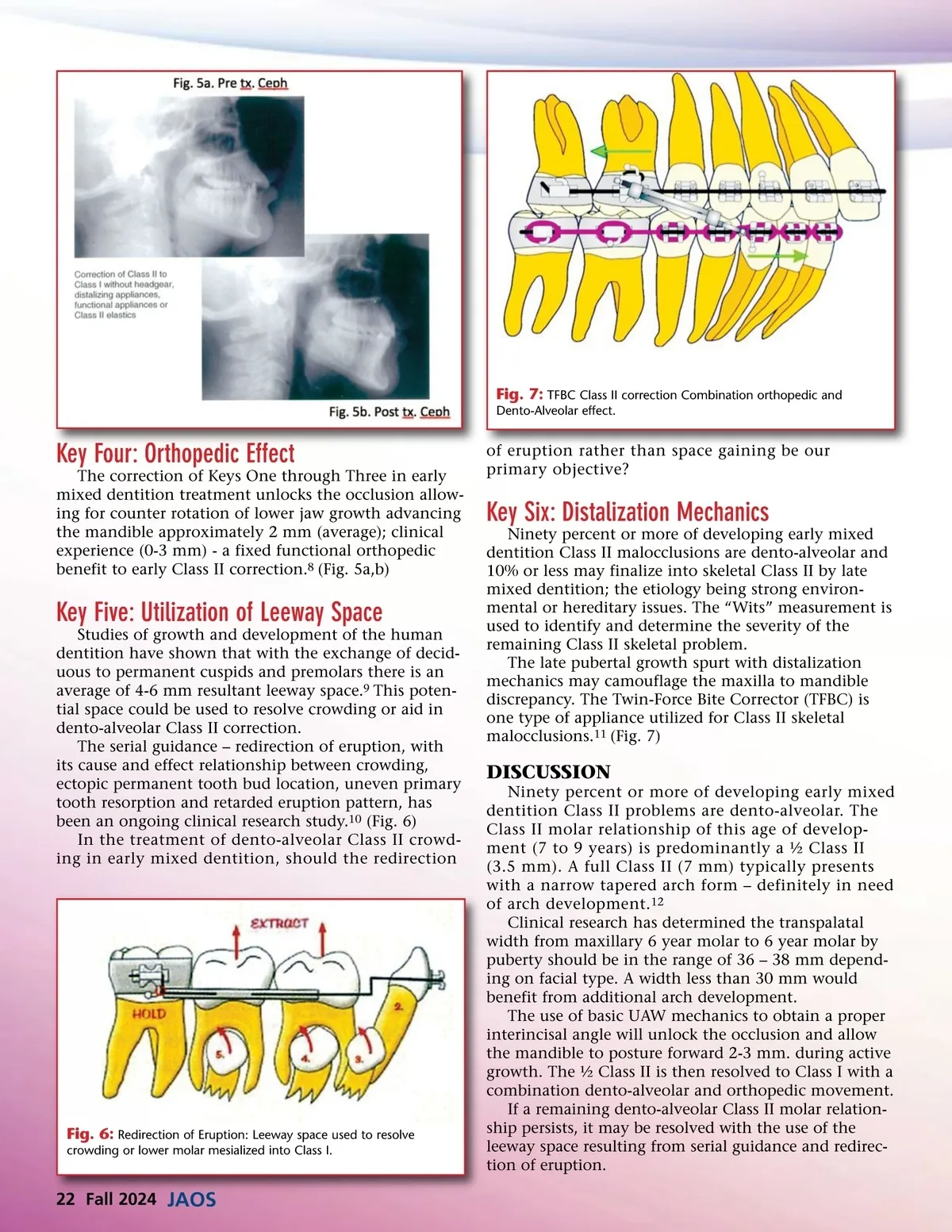
Fig. 7: TFBC Class II correction Combination orthopedic and Dento-Alveolar effect. Key Four: Orthopedic Effect The correction of Keys One through Three in early mixed dentition treatment unlocks the occlusion allow-ing for counter rotation of lower jaw growth advancing the mandible approximately 2 mm (average); clinical experience (0-3 mm) -a fixed functional orthopedic benefit to early Class II correction. 8 (Fig. 5a,b) of eruption rather than space gaining be our primary objective? Key Six: Distalization Mechanics Ninety percent or more of developing early mixed dentition Class II malocclusions are dento-alveolar and 10% or less may finalize into skeletal Class II by late mixed dentition; the etiology being strong environ-mental or hereditary issues. The “Wits” measurement is used to identify and determine the severity of the remaining Class II skeletal problem. The late pubertal growth spurt with distalization mechanics may camouflage the maxilla to mandible discrepancy. The Twin-Force Bite Corrector (TFBC) is one type of appliance utilized for Class II skeletal malocclusions. 11 (Fig. 7) Key Five: Utilization of Leeway Space Studies of growth and development of the human dentition have shown that with the exchange of decid-uous to permanent cuspids and premolars there is an average of 4-6 mm resultant leeway space. 9 This poten-tial space could be used to resolve crowding or aid in dento-alveolar Class II correction. The serial guidance – redirection of eruption, with its cause and effect relationship between crowding, ectopic permanent tooth bud location, uneven primary tooth resorption and retarded eruption pattern, has been an ongoing clinical research study. 10 (Fig. 6) In the treatment of dento-alveolar Class II crowd-ing in early mixed dentition, should the redirection DISCUSSION Ninety percent or more of developing early mixed dentition Class II problems are dento-alveolar. The Class II molar relationship of this age of develop-ment (7 to 9 years) is predominantly a ½ Class II (3.5 mm). A full Class II (7 mm) typically presents with a narrow tapered arch form – definitely in need of arch development. 12 Clinical research has determined the transpalatal width from maxillary 6 year molar to 6 year molar by puberty should be in the range of 36 – 38 mm depend-ing on facial type. A width less than 30 mm would benefit from additional arch development. The use of basic UAW mechanics to obtain a proper interincisal angle will unlock the occlusion and allow the mandible to posture forward 2-3 mm. during active growth. The ½ Class II is then resolved to Class I with a combination dento-alveolar and orthopedic movement. If a remaining dento-alveolar Class II molar relation-ship persists, it may be resolved with the use of the leeway space resulting from serial guidance and redirec-tion of eruption. Fig. 6: Redirection of Eruption: Leeway space used to resolve crowding or lower molar mesialized into Class I. 22 Fall 2024 JAOS
Journal of the American Orthodontic Society Fall 2024: Page 22