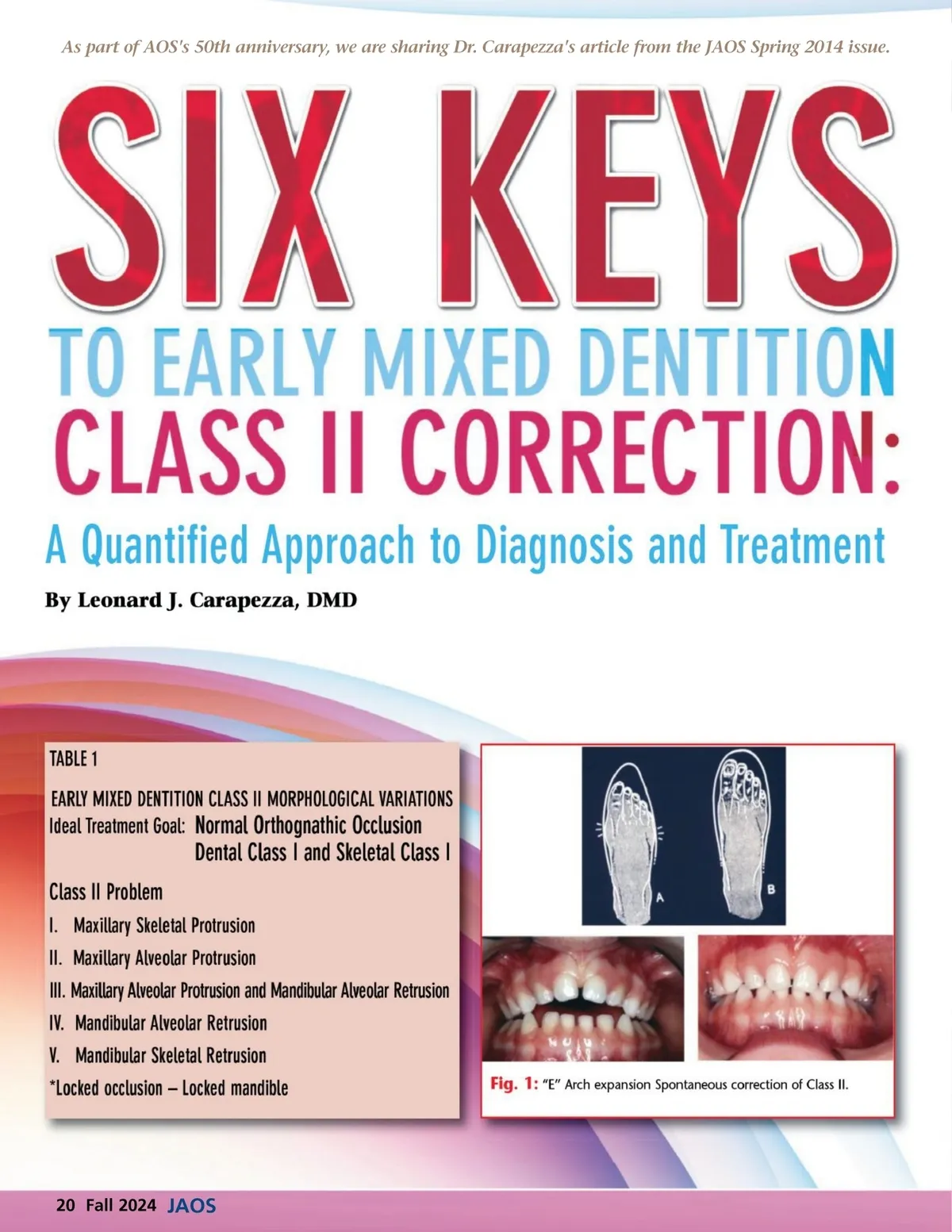
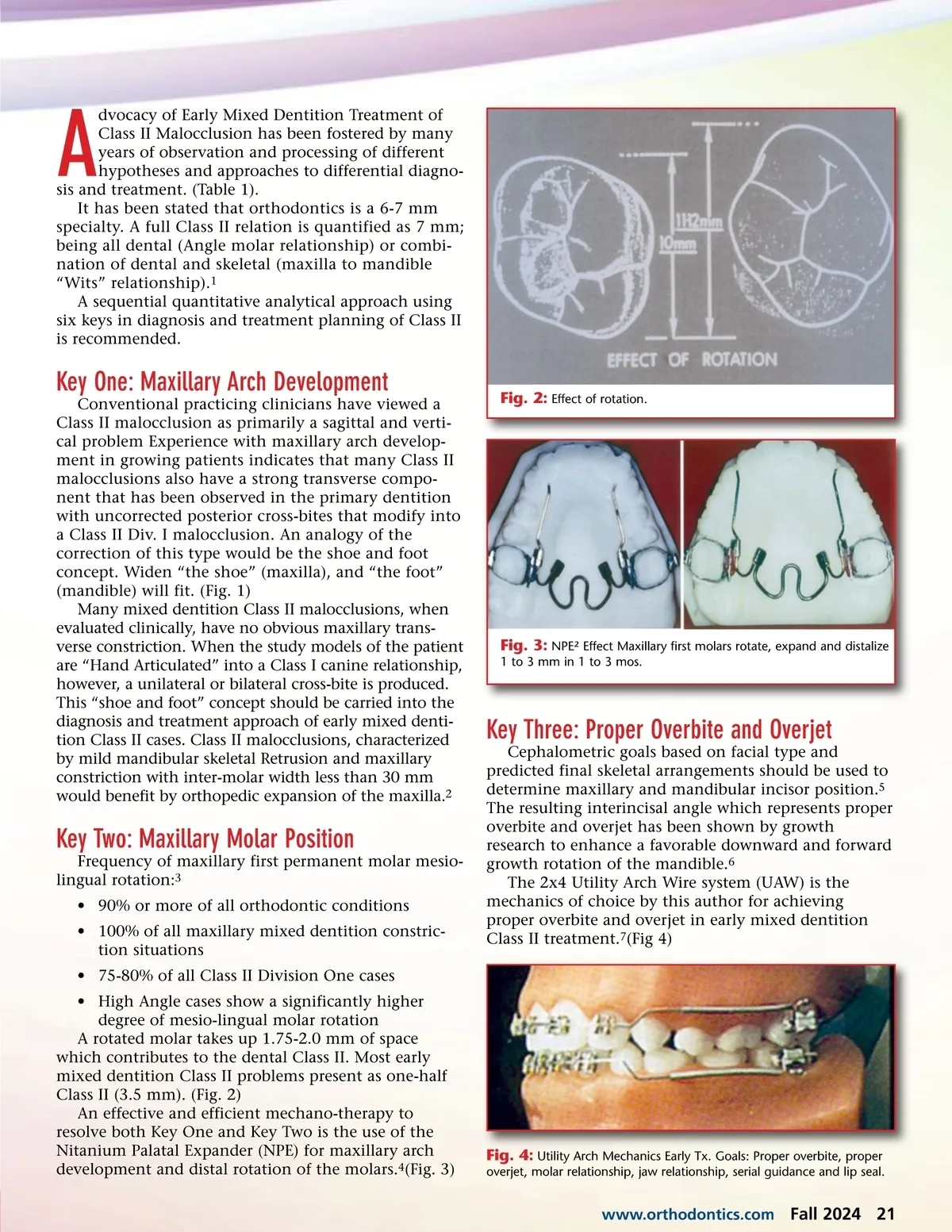
dvocacy of Early Mixed Dentition Treatment of Class II Malocclusion has been fostered by many years of observation and processing of different hypotheses and approaches to differential diagno-sis and treatment. (Table 1). It has been stated that orthodontics is a 6-7 mm specialty. A full Class II relation is quantified as 7 mm; being all dental (Angle molar relationship) or combi-nation of dental and skeletal (maxilla to mandible “Wits” relationship). 1 A sequential quantitative analytical approach using six keys in diagnosis and treatment planning of Class II is recommended. A Key One: Maxillary Arch Development Conventional practicing clinicians have viewed a Class II malocclusion as primarily a sagittal and verti-cal problem Experience with maxillary arch develop-ment in growing patients indicates that many Class II malocclusions also have a strong transverse compo-nent that has been observed in the primary dentition with uncorrected posterior cross-bites that modify into a Class II Div. I malocclusion. An analogy of the correction of this type would be the shoe and foot concept. Widen “the shoe” (maxilla), and “the foot” (mandible) will fit. (Fig. 1) Many mixed dentition Class II malocclusions, when evaluated clinically, have no obvious maxillary trans-verse constriction. When the study models of the patient are “Hand Articulated” into a Class I canine relationship, however, a unilateral or bilateral cross-bite is produced. This “shoe and foot” concept should be carried into the diagnosis and treatment approach of early mixed denti-tion Class II cases. Class II malocclusions, characterized by mild mandibular skeletal Retrusion and maxillary constriction with inter-molar width less than 30 mm would benefit by orthopedic expansion of the maxilla. 2 Fig. 2: Effect of rotation. Fig. 3: NPE² Effect Maxillary first molars rotate, expand and distalize 1 to 3 mm in 1 to 3 mos. Key Three: Proper Overbite and Overjet Cephalometric goals based on facial type and predicted final skeletal arrangements should be used to determine maxillary and mandibular incisor position. 5 The resulting interincisal angle which represents proper overbite and overjet has been shown by growth research to enhance a favorable downward and forward growth rotation of the mandible. 6 The 2x4 Utility Arch Wire system (UAW) is the mechanics of choice by this author for achieving proper overbite and overjet in early mixed dentition Class II treatment. 7 (Fig 4) Key Two: Maxillary Molar Position Frequency of maxillary first permanent molar mesio-lingual rotation: 3 • 90% or more of all orthodontic conditions • 100% of all maxillary mixed dentition constric-tion situations • 75-80% of all Class II Division One cases • High Angle cases show a significantly higher degree of mesio-lingual molar rotation A rotated molar takes up 1.75-2.0 mm of space which contributes to the dental Class II. Most early mixed dentition Class II problems present as one-half Class II (3.5 mm). (Fig. 2) An effective and efficient mechano-therapy to resolve both Key One and Key Two is the use of the Nitanium Palatal Expander (NPE) for maxillary arch development and distal rotation of the molars. 4 (Fig. 3) Fig. 4: Utility Arch Mechanics Early Tx. Goals: Proper overbite, proper overjet, molar relationship, jaw relationship, serial guidance and lip seal. www.orthodontics.com Fall 2024 21
Journal of the American Orthodontic Society Fall 2024: Page 21