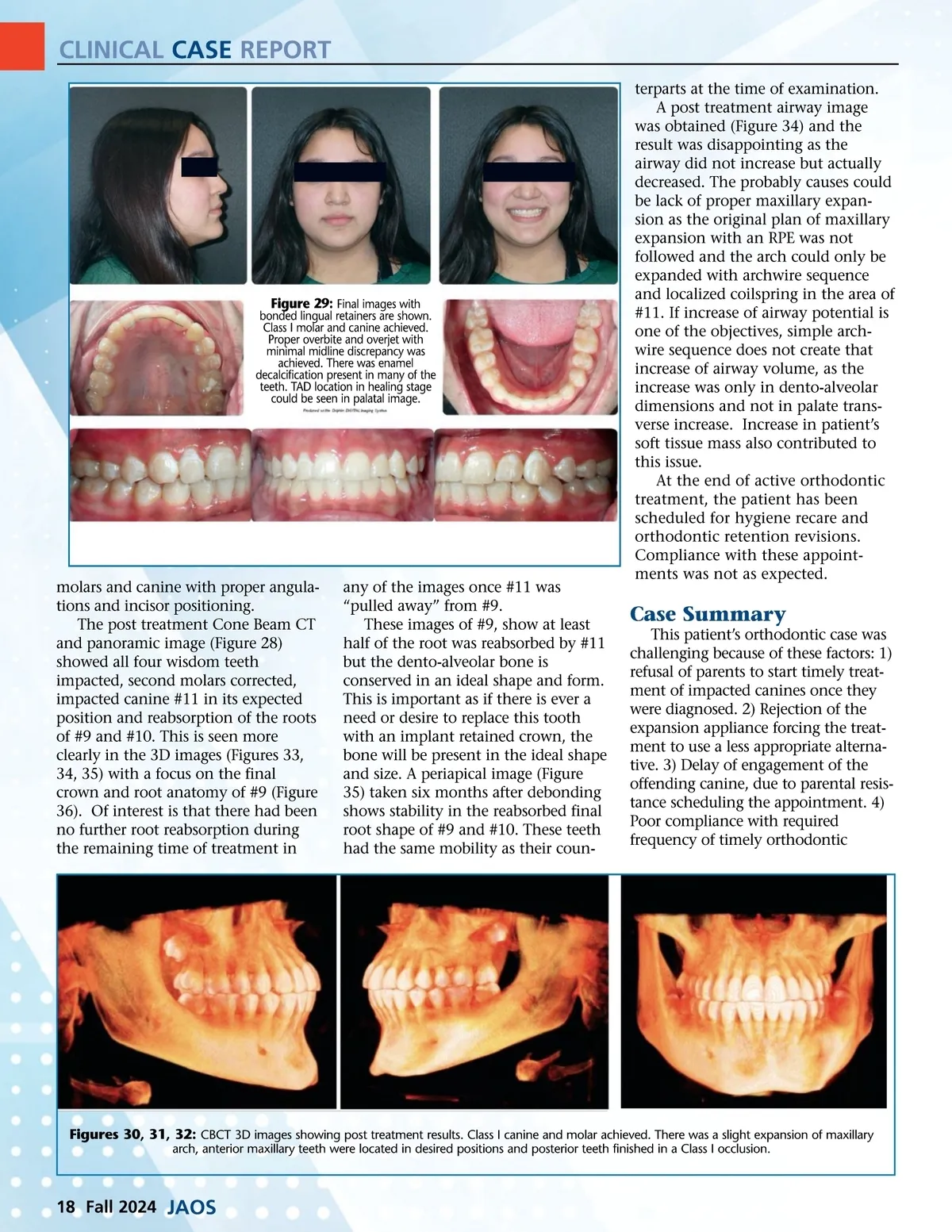
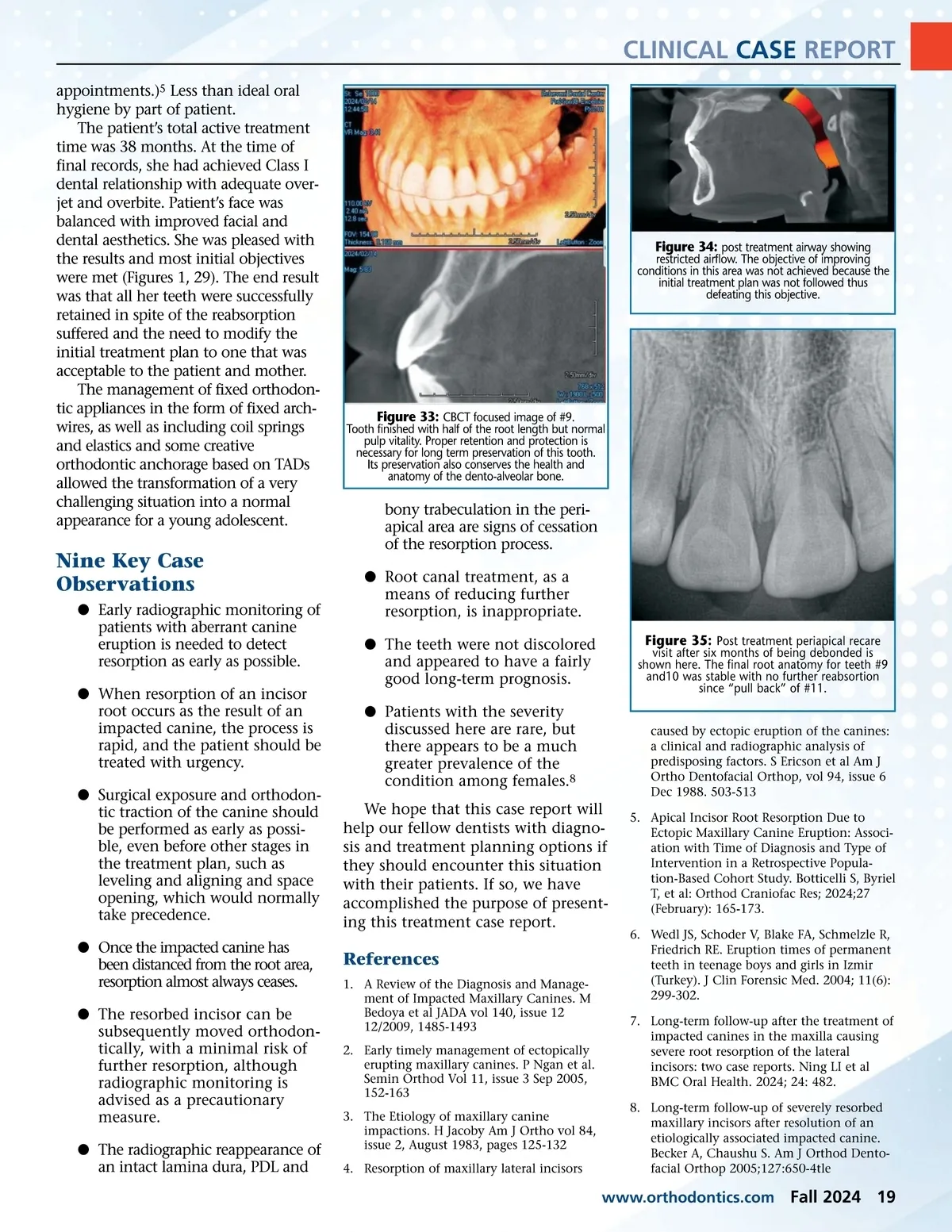
CLINICAL CASE REPORT terparts at the time of examination. A post treatment airway image was obtained (Figure 34) and the result was disappointing as the airway did not increase but actually decreased. The probably causes could be lack of proper maxillary expan-sion as the original plan of maxillary expansion with an RPE was not followed and the arch could only be expanded with archwire sequence and localized coilspring in the area of #11. If increase of airway potential is one of the objectives, simple arch-wire sequence does not create that increase of airway volume, as the increase was only in dento-alveolar dimensions and not in palate trans-verse increase. Increase in patient’s soft tissue mass also contributed to this issue. At the end of active orthodontic treatment, the patient has been scheduled for hygiene recare and orthodontic retention revisions. Compliance with these appoint-ments was not as expected. Figure 29: Final images with bonded lingual retainers are shown. Class I molar and canine achieved. Proper overbite and overjet with minimal midline discrepancy was achieved. There was enamel decalcification present in many of the teeth. TAD location in healing stage could be seen in palatal image. molars and canine with proper angula-tions and incisor positioning. The post treatment Cone Beam CT and panoramic image (Figure 28) showed all four wisdom teeth impacted, second molars corrected, impacted canine #11 in its expected position and reabsorption of the roots of #9 and #10. This is seen more clearly in the 3D images (Figures 33, 34, 35) with a focus on the final crown and root anatomy of #9 (Figure 36). Of interest is that there had been no further root reabsorption during the remaining time of treatment in any of the images once #11 was “pulled away” from #9. These images of #9, show at least half of the root was reabsorbed by #11 but the dento-alveolar bone is conserved in an ideal shape and form. This is important as if there is ever a need or desire to replace this tooth with an implant retained crown, the bone will be present in the ideal shape and size. A periapical image (Figure 35) taken six months after debonding shows stability in the reabsorbed final root shape of #9 and #10. These teeth had the same mobility as their coun-Case Summary This patient’s orthodontic case was challenging because of these factors: 1) refusal of parents to start timely treat-ment of impacted canines once they were diagnosed. 2) Rejection of the expansion appliance forcing the treat-ment to use a less appropriate alterna-tive. 3) Delay of engagement of the offending canine, due to parental resis-tance scheduling the appointment. 4) Poor compliance with required frequency of timely orthodontic Figures 30, 31, 32: CBCT 3D images showing post treatment results. Class I canine and molar achieved. There was a slight expansion of maxillary arch, anterior maxillary teeth were located in desired positions and posterior teeth finished in a Class I occlusion. 18 Fall 2024 JAOS
Journal of the American Orthodontic Society Fall 2024: Page 18