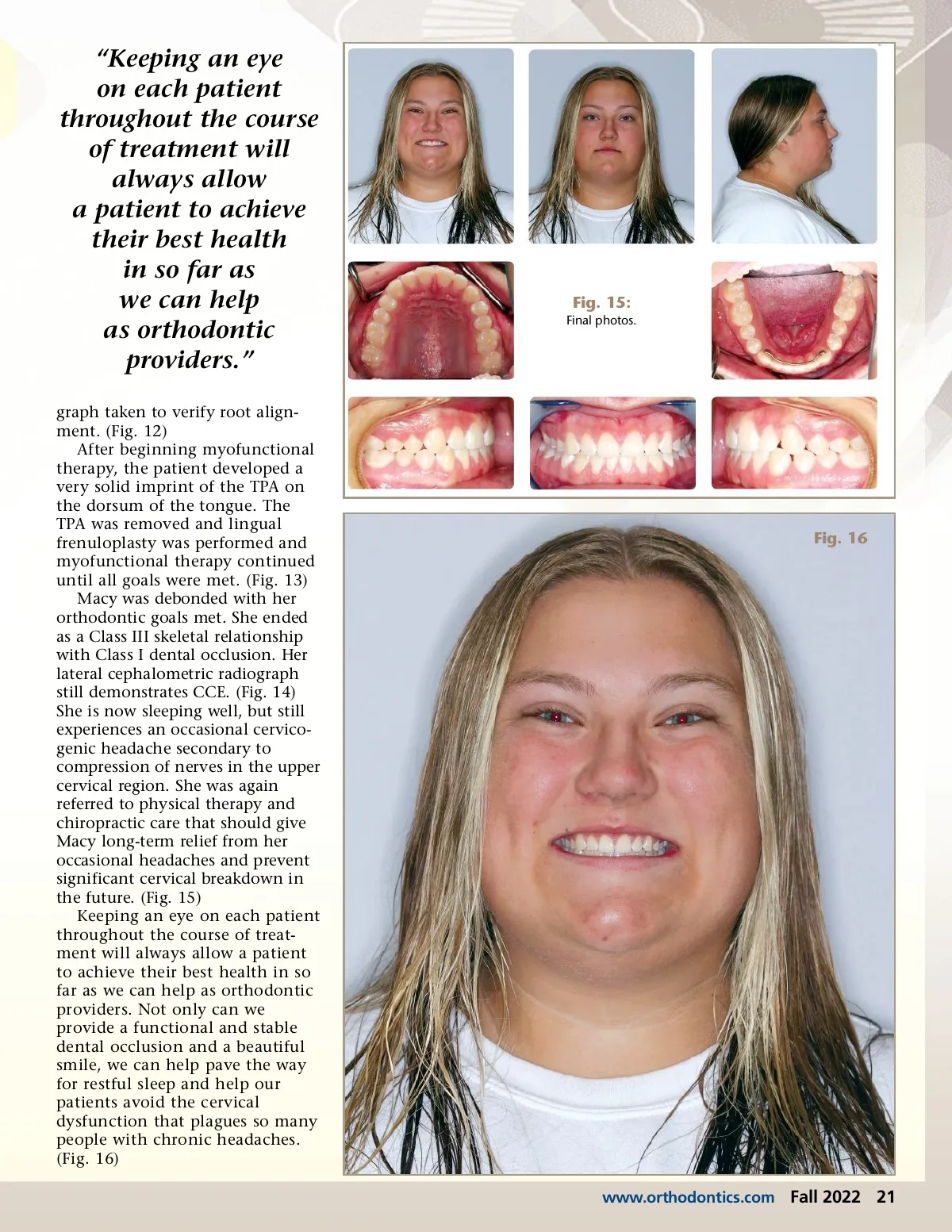
Fig. 13: Post-lingual frenuloplasty surgery. accomplished prior to correcting tongue tie, tongue posture and function. Conversely, taking a child through a tongue-tie release and myofunctional therapy to establish normal tongue posture and swallow, and then placing such an appliance in the mouth can be very disruptive to the child and interfere with goals of myofunctional therapy and the results that may be achieved. Evaluation of the tongue tie is critical in determining whether it is necessary to release or should be monitored. Numerous diagnostic criteria are used in this process with evaluation of both functional abil-ity and deficiency as well as physi-cal characteristics of the frenum and other adaptive patterns of dysfunction the patient is experi-encing. If the patient indeed suffers from ankyloglossia, one must evalu-ate tongue tie, tongue space and tongue tone before considering myofunctional therapy and a release. If the patient has inade-quate tongue space, a releasing tongue surgery will not provide significant benefit for the patient, nor will the optimal results be achieved post-surgically. Patients with inadequate tongue space must first have tongue space created. This is most successfully achieved through orthodontic expansion techniques that influ-ence the maxilla and supporting dentoalveolar bone of the maxilla and mandible. Tongue tone is also a very important consideration, as a patient with low tongue strength will not respond well to a tongue-tie release. The tongue simply does not have enough strength to perform the necessary rehabilitation and will end with a less-than-opti-Fig. 14: Final lateral ceph. mal post-surgical result. It has been said that a patient will go through a tongue-tie release once, but will not look forward to a second time. Treatment goals for Macy were the following: e. Revisit nasal airway, sleep and headaches Macy began with the insert of her RPE appliance that was acti-vated once a day until 6 mm of expansion was achieved. (Fig. 8) At two months, after full expansion (Fig. 9), the RPE was removed, bands on the upper 6’s were replaced and a molar rotator was attempted to be placed. However, due to palatal anatomy, it was not possible to place, so a transpalatal arch TPA was fabricated (Fig. 10) to allow maintenance of the expanded dimension of the upper arch and to distal rotate the upper molars. At five months, the upper and lower arches were bonded 7-7 and a temporary pad was placed on the LL6 for bracket clearance. Light upper and lower nitanium arch wires were placed. The patient continued with a straight wire series until she was in U/L 19x25TN wires at 14 months. (Fig. 11) She stated at this visit how much better her sleep had become since we began her treat-ment. Bilateral posterior box elas-tics to close the open bite were placed and, at 19 months, the patient was referred to a myofunc-tional therapist for evaluation of her tongue-tie and tongue thrust swallow. Stable MIP has been achieved and a panoramic radio-ᕡ Establish normal nasal breathing a. Saline nasal spray b. Allergy evaluation c. Rapid palatal expansion (RPE) ᕢ Myofunctional evaluation of the tongue tie and dysfunctional swallow a. Manage tongue tie and tongue thrust after RPE and during braces phase ᕣ Physical therapy/chiropractic evaluation for cervical dysfunc-tion and loss of lordotic curve ᕤ Expand the maxilla with RPE and distal rotate the upper molars towards a Class I relation-ship ᕥ Re-evaluate nasal breathing, sleep and headaches ᕦ SWS to finish a. Band and bond upper and lower arches b. Begin MF therapy and prepare patient for tongue tie release c. Class II mechanics as needed d. Retention of case 20 Fall 2022 JAOS
Journal of the American Orthodontic Society Fall 2022: Page 20