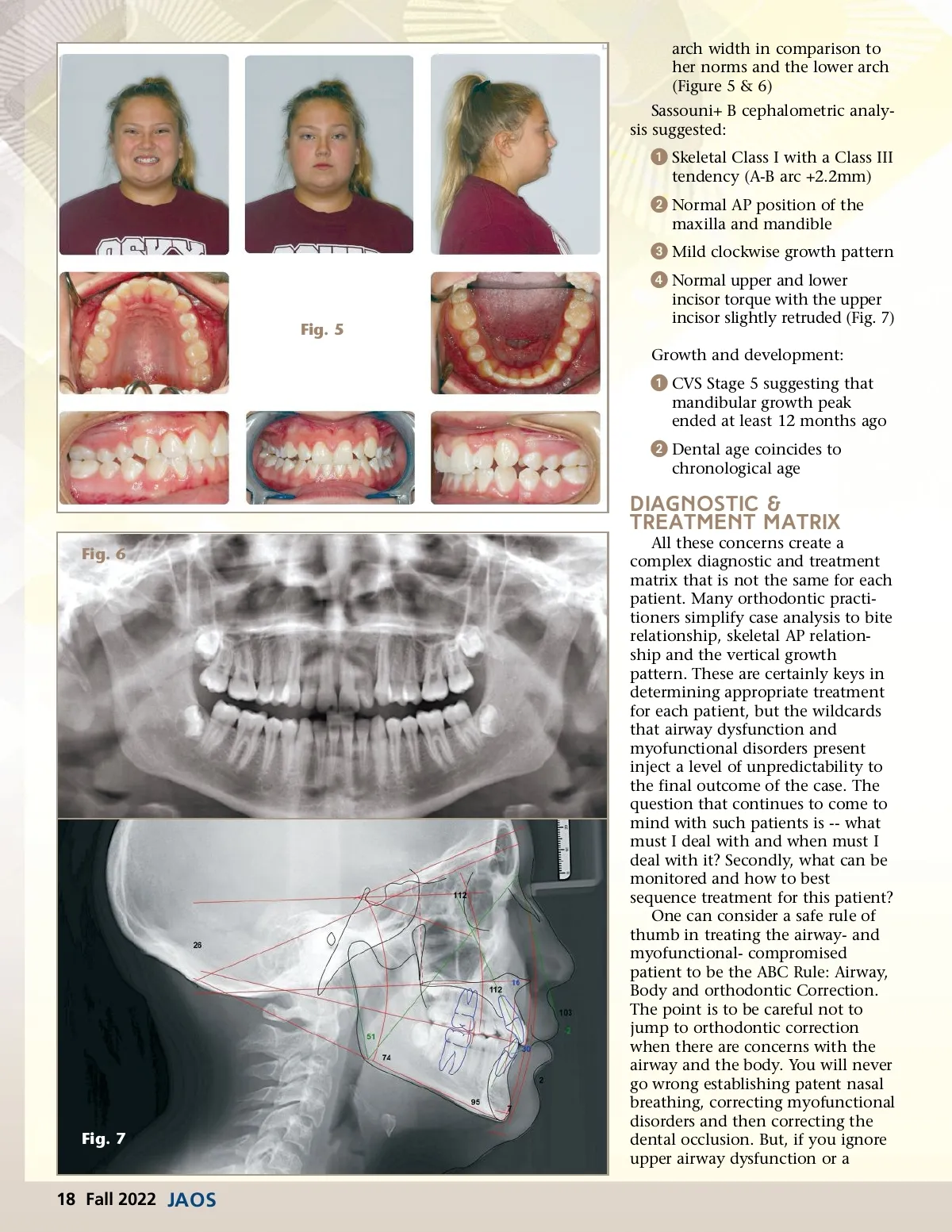
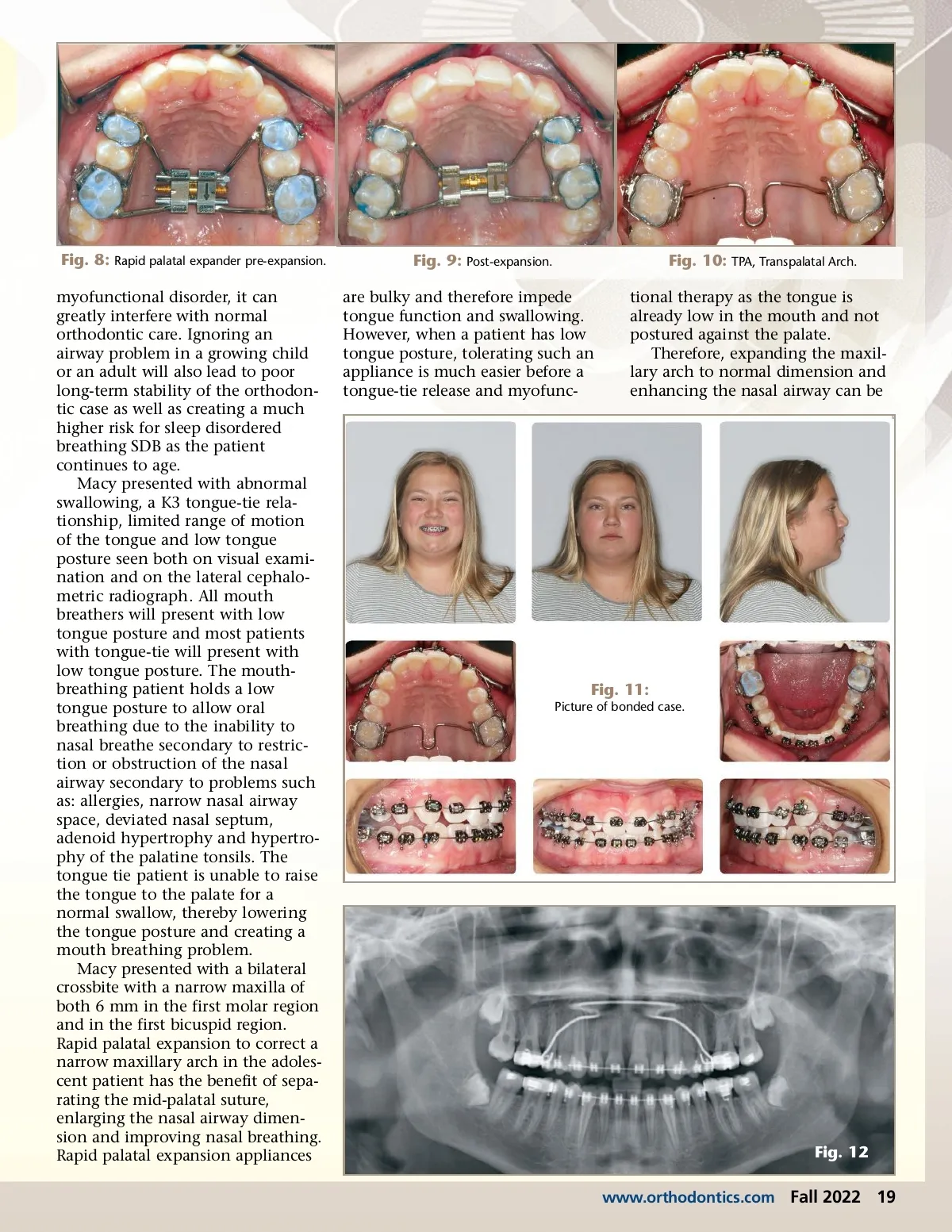
Fig. 8: Rapid palatal expander pre-expansion. myofunctional disorder, it can greatly interfere with normal orthodontic care. Ignoring an airway problem in a growing child or an adult will also lead to poor long-term stability of the orthodon-tic case as well as creating a much higher risk for sleep disordered breathing SDB as the patient continues to age. Macy presented with abnormal swallowing, a K3 tongue-tie rela-tionship, limited range of motion of the tongue and low tongue posture seen both on visual exami-nation and on the lateral cephalo-metric radiograph. All mouth breathers will present with low tongue posture and most patients with tongue-tie will present with low tongue posture. The mouth-breathing patient holds a low tongue posture to allow oral breathing due to the inability to nasal breathe secondary to restric-tion or obstruction of the nasal airway secondary to problems such as: allergies, narrow nasal airway space, deviated nasal septum, adenoid hypertrophy and hypertro-phy of the palatine tonsils. The tongue tie patient is unable to raise the tongue to the palate for a normal swallow, thereby lowering the tongue posture and creating a mouth breathing problem. Macy presented with a bilateral crossbite with a narrow maxilla of both 6 mm in the first molar region and in the first bicuspid region. Rapid palatal expansion to correct a narrow maxillary arch in the adoles-cent patient has the benefit of sepa-rating the mid-palatal suture, enlarging the nasal airway dimen-sion and improving nasal breathing. Rapid palatal expansion appliances Fig. 9: Post-expansion. are bulky and therefore impede tongue function and swallowing. However, when a patient has low tongue posture, tolerating such an appliance is much easier before a tongue-tie release and myofunc-Fig. 10: TPA, Transpalatal Arch. tional therapy as the tongue is already low in the mouth and not postured against the palate. Therefore, expanding the maxil-lary arch to normal dimension and enhancing the nasal airway can be Fig. 11: Picture of bonded case. Fig. 12 www.orthodontics.com Fall 2022 19
Journal of the American Orthodontic Society Fall 2022: Page 19