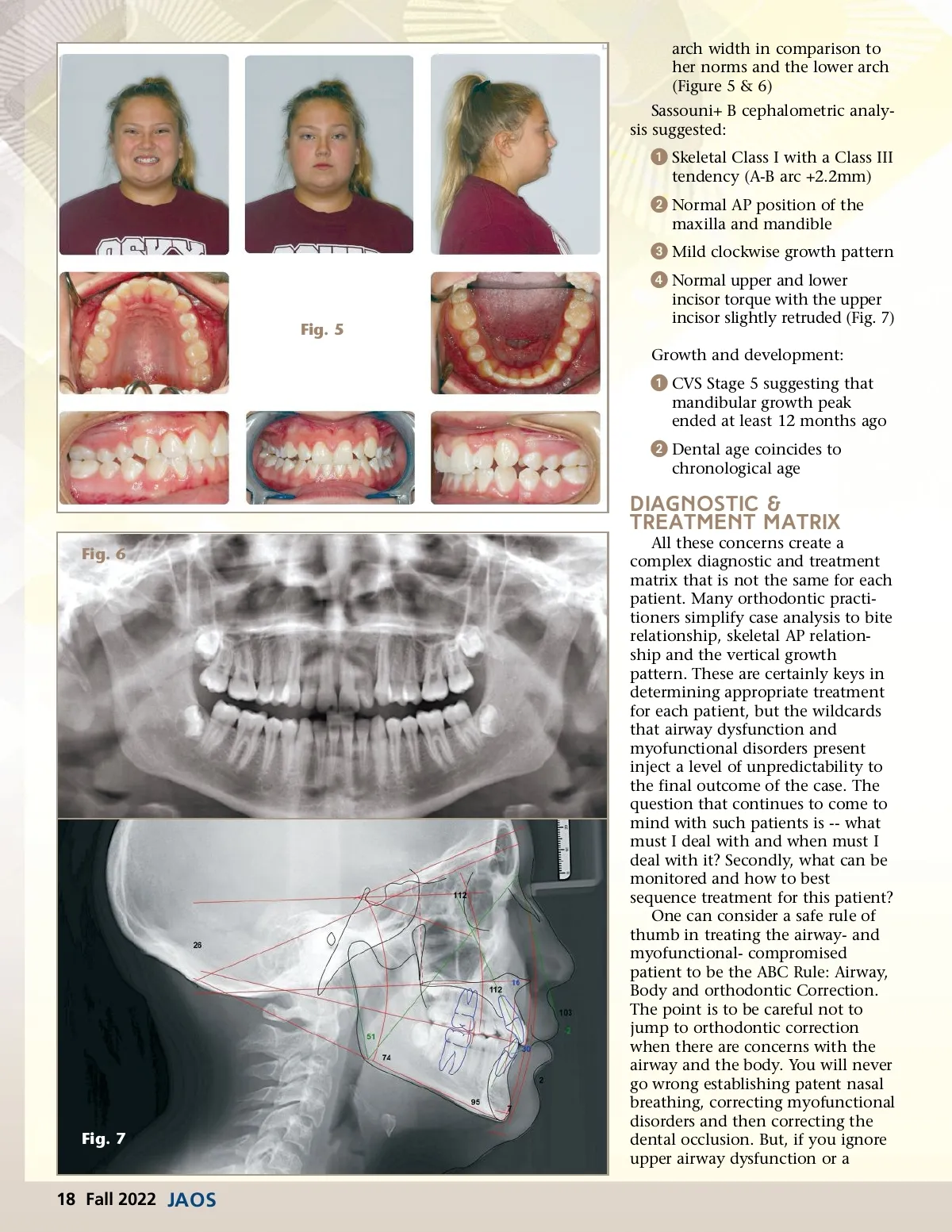
arch width in comparison to her norms and the lower arch (Figure 5 & 6) Sassouni+ B cephalometric analy-sis suggested: ᕡ Skeletal Class I with a Class III tendency (A-B arc +2.2mm) ᕢ Normal AP position of the maxilla and mandible ᕣ Mild clockwise growth pattern ᕤ Normal upper and lower Fig. 5 incisor torque with the upper incisor slightly retruded (Fig. 7) Growth and development: ᕡ CVS Stage 5 suggesting that mandibular growth peak ended at least 12 months ago ᕢ Dental age coincides to chronological age Diagnostic & Treatment Matrix Fig. 6 Fig. 7 All these concerns create a complex diagnostic and treatment matrix that is not the same for each patient. Many orthodontic practi-tioners simplify case analysis to bite relationship, skeletal AP relation-ship and the vertical growth pattern. These are certainly keys in determining appropriate treatment for each patient, but the wildcards that airway dysfunction and myofunctional disorders present inject a level of unpredictability to the final outcome of the case. The question that continues to come to mind with such patients is --what must I deal with and when must I deal with it? Secondly, what can be monitored and how to best sequence treatment for this patient? One can consider a safe rule of thumb in treating the airway-and myofunctional-compromised patient to be the ABC Rule: Airway, Body and orthodontic Correction. The point is to be careful not to jump to orthodontic correction when there are concerns with the airway and the body. You will never go wrong establishing patent nasal breathing, correcting myofunctional disorders and then correcting the dental occlusion. But, if you ignore upper airway dysfunction or a 18 Fall 2022 JAOS
Journal of the American Orthodontic Society Fall 2022: Page 18