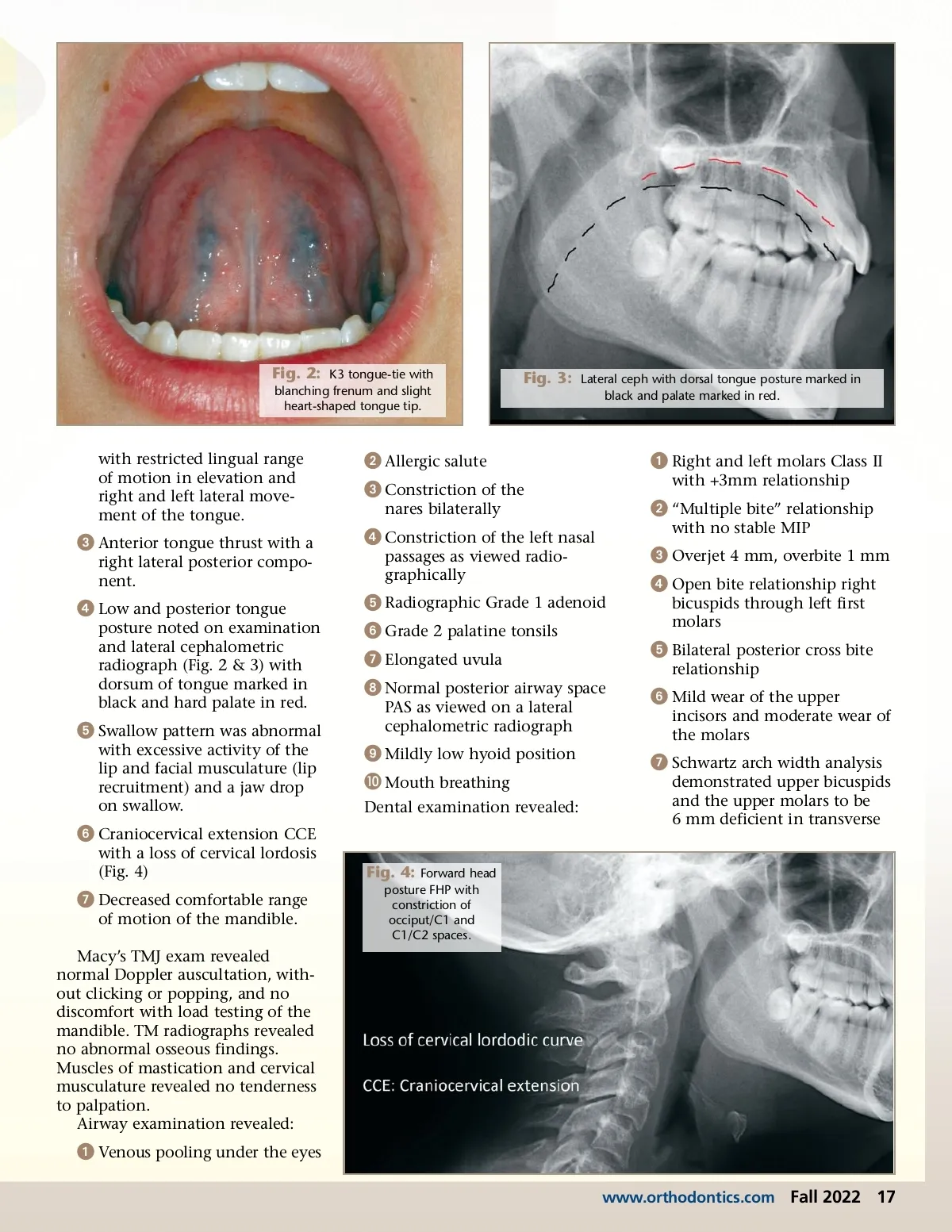
Fig. 2: K3 tongue-tie with blanching frenum and slight heart-shaped tongue tip. Fig. 3: Lateral ceph with dorsal tongue posture marked in black and palate marked in red. with restricted lingual range of motion in elevation and right and left lateral move-ment of the tongue. ᕢ Allergic salute ᕣ Constriction of the nares bilaterally ᕡ Right and left molars Class II with +3mm relationship ᕢ “Multiple bite” relationship with no stable MIP ᕣ Anterior tongue thrust with a right lateral posterior compo-nent. ᕤ Constriction of the left nasal passages as viewed radio-graphically ᕣ Overjet 4 mm, overbite 1 mm ᕤ Open bite relationship right bicuspids through left first molars ᕤ Low and posterior tongue posture noted on examination and lateral cephalometric radiograph (Fig. 2 & 3) with dorsum of tongue marked in black and hard palate in red. ᕥ Radiographic Grade 1 adenoid ᕦ Grade 2 palatine tonsils ᕧ Elongated uvula ᕨ Normal posterior airway space PAS as viewed on a lateral cephalometric radiograph ᕥ Bilateral posterior cross bite relationship ᕦ Mild wear of the upper incisors and moderate wear of the molars ᕥ Swallow pattern was abnormal with excessive activity of the lip and facial musculature (lip recruitment) and a jaw drop on swallow. ᕩ Mildly low hyoid position µ Mouth breathing Dental examination revealed: ᕧ Schwartz arch width analysis demonstrated upper bicuspids and the upper molars to be 6 mm deficient in transverse ᕦ Craniocervical extension CCE with a loss of cervical lordosis (Fig. 4) Fig. 4: Forward head posture FHP with constriction of occiput/C1 and C1/C2 spaces. ᕧ Decreased comfortable range of motion of the mandible. Macy’s TMJ exam revealed normal Doppler auscultation, with-out clicking or popping, and no discomfort with load testing of the mandible. TM radiographs revealed no abnormal osseous findings. Muscles of mastication and cervical musculature revealed no tenderness to palpation. Airway examination revealed: ᕡ Venous pooling under the eyes www.orthodontics.com Fall 2022 17
Journal of the American Orthodontic Society Fall 2022: Page 17