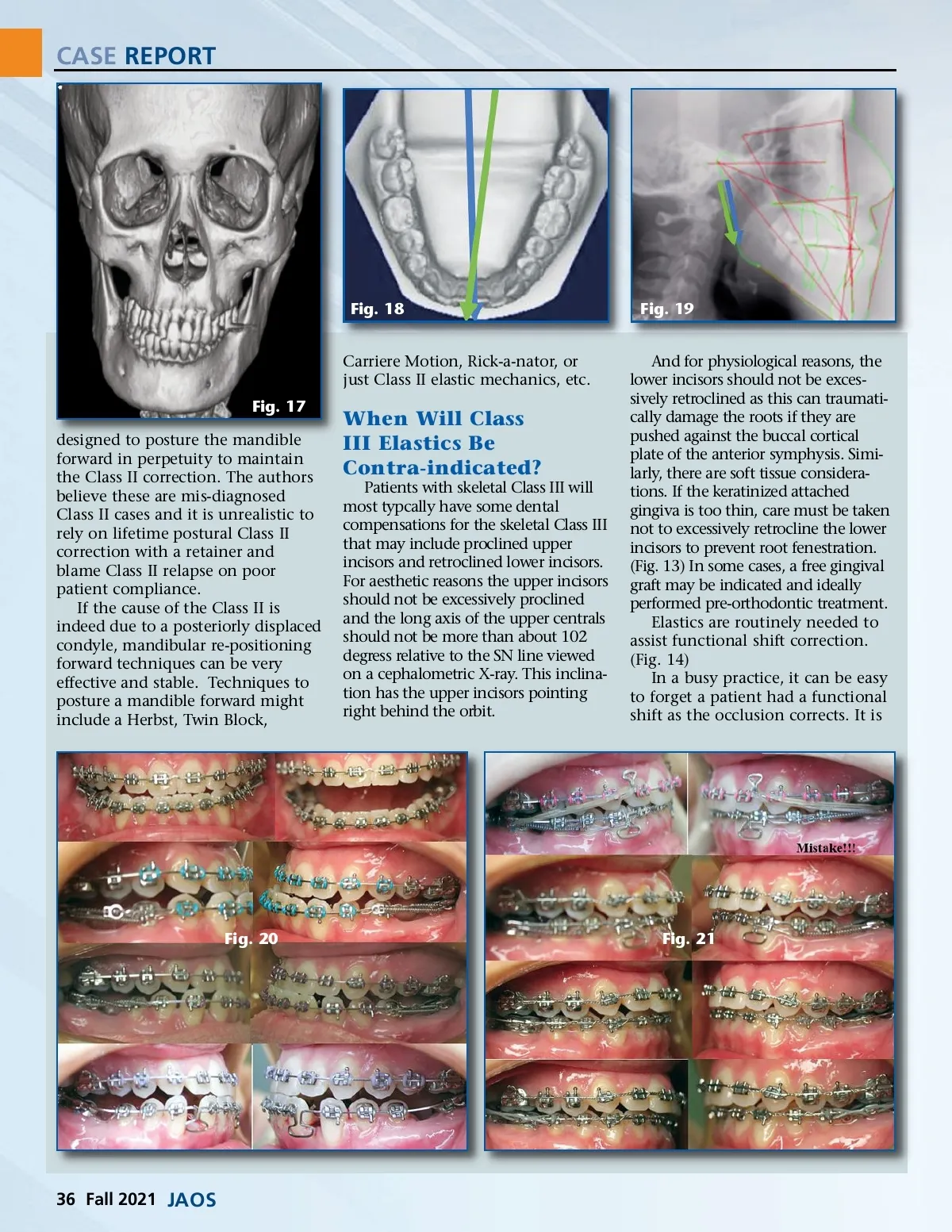
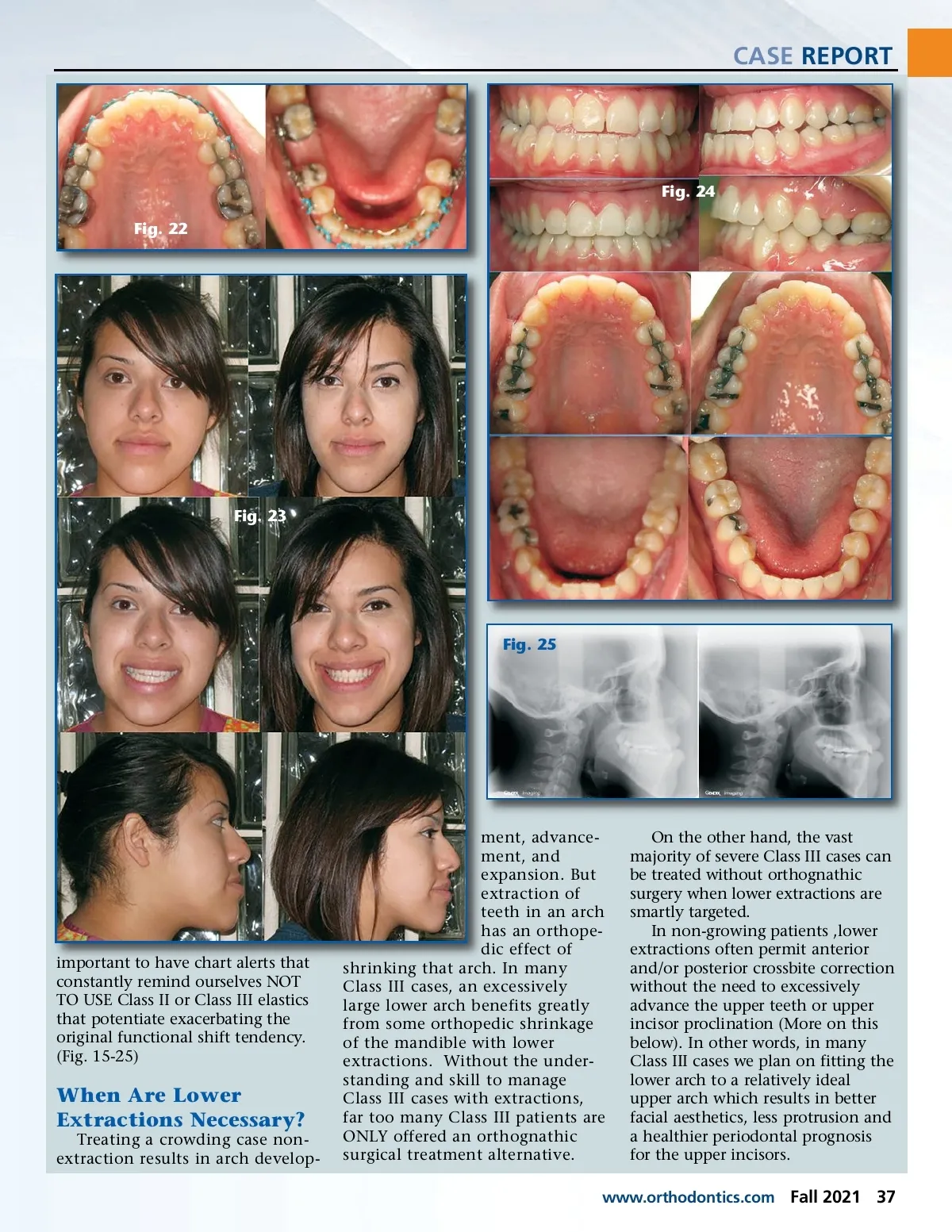
CASE REPORT Fig. 18 Carriere Motion, Rick-a-nator, or just Class II elastic mechanics, etc. Fig. 17 designed to posture the mandible forward in perpetuity to maintain the Class II correction. The authors believe these are mis-diagnosed Class II cases and it is unrealistic to rely on lifetime postural Class II correction with a retainer and blame Class II relapse on poor patient compliance. If the cause of the Class II is indeed due to a posteriorly displaced condyle, mandibular re-positioning forward techniques can be very effective and stable. Techniques to posture a mandible forward might include a Herbst, Twin Block, Fig. 19 And for physiological reasons, the lower incisors should not be exces-sively retroclined as this can traumati-cally damage the roots if they are pushed against the buccal cortical plate of the anterior symphysis. Simi-larly, there are soft tissue considera-tions. If the keratinized attached gingiva is too thin, care must be taken not to excessively retrocline the lower incisors to prevent root fenestration. (Fig. 13) In some cases, a free gingival graft may be indicated and ideally performed pre-orthodontic treatment. Elastics are routinely needed to assist functional shift correction. (Fig. 14) In a busy practice, it can be easy to forget a patient had a functional shift as the occlusion corrects. It is When Will Class III Elastics Be Contra-indicated? Patients with skeletal Class III will most typcally have some dental compensations for the skeletal Class III that may include proclined upper incisors and retroclined lower incisors. For aesthetic reasons the upper incisors should not be excessively proclined and the long axis of the upper centrals should not be more than about 102 degress relative to the SN line viewed on a cephalometric X-ray. This inclina-tion has the upper incisors pointing right behind the orbit. Fig. 20 Fig. 21 36 Fall 2021 JAOS
Journal of the American Orthodontic Society Fall 2021: Page 36