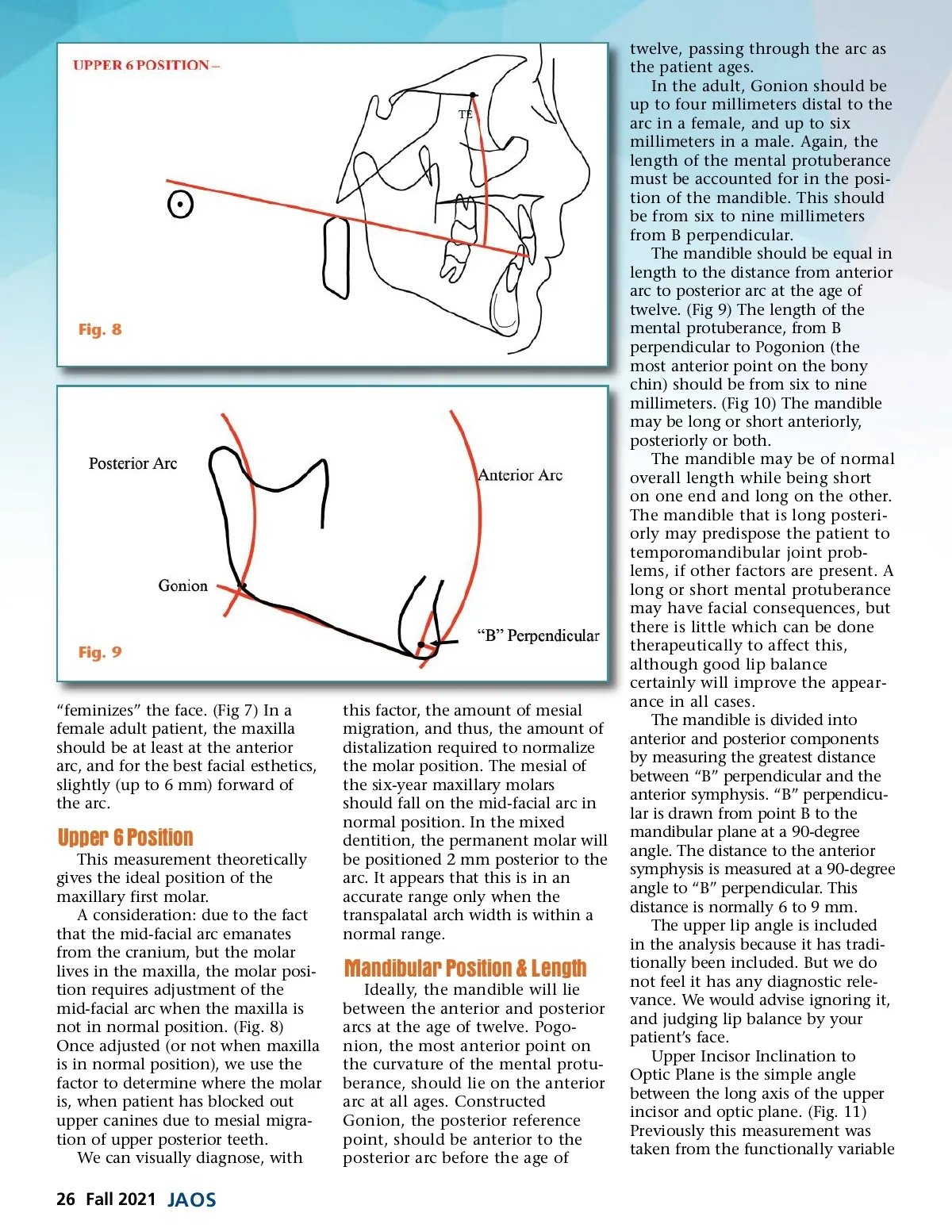
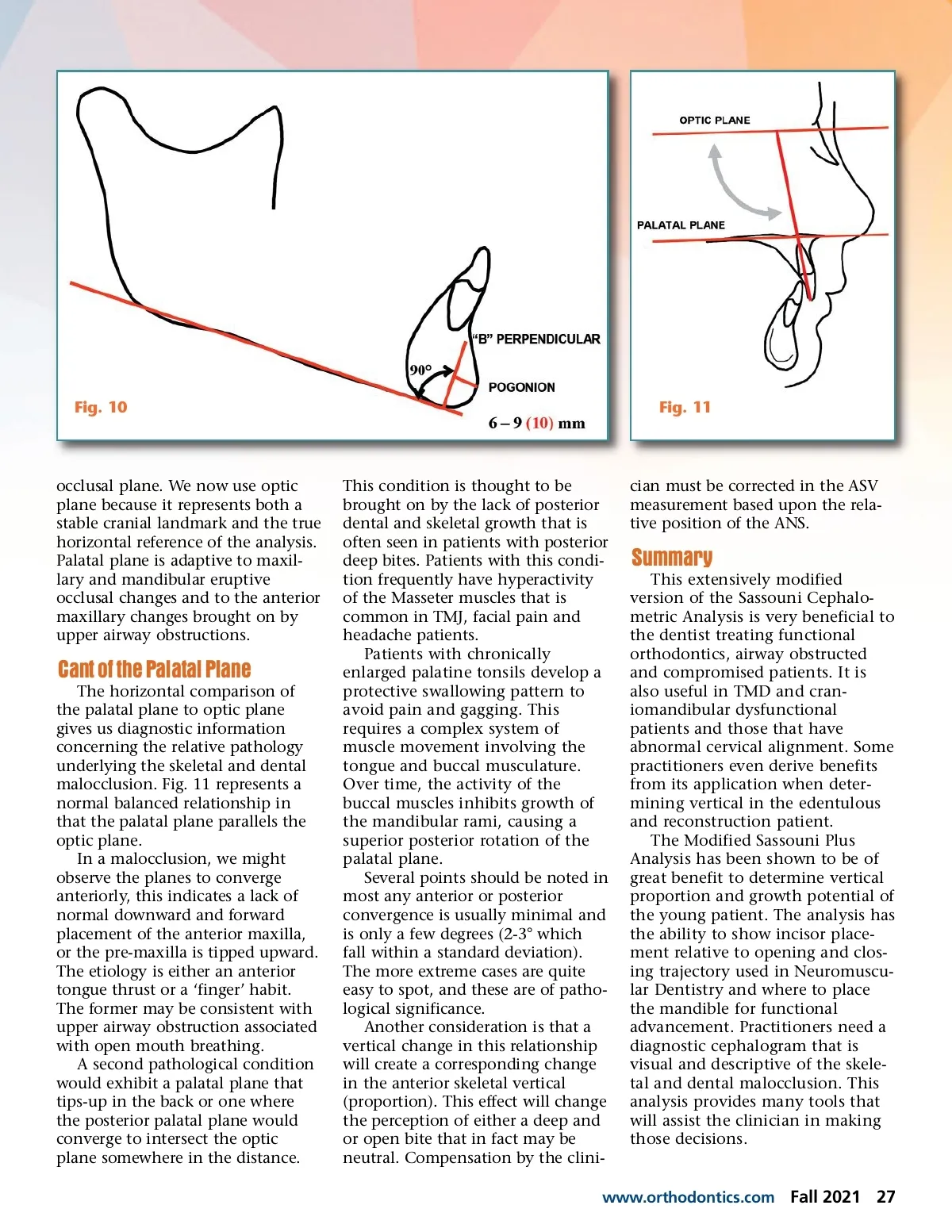
Fig. 10 Fig. 11 occlusal plane. We now use optic plane because it represents both a stable cranial landmark and the true horizontal reference of the analysis. Palatal plane is adaptive to maxil-lary and mandibular eruptive occlusal changes and to the anterior maxillary changes brought on by upper airway obstructions. Cant of the Palatal Plane The horizontal comparison of the palatal plane to optic plane gives us diagnostic information concerning the relative pathology underlying the skeletal and dental malocclusion. Fig. 11 represents a normal balanced relationship in that the palatal plane parallels the optic plane. In a malocclusion, we might observe the planes to converge anteriorly, this indicates a lack of normal downward and forward placement of the anterior maxilla, or the pre-maxilla is tipped upward. The etiology is either an anterior tongue thrust or a ‘finger’ habit. The former may be consistent with upper airway obstruction associated with open mouth breathing. A second pathological condition would exhibit a palatal plane that tips-up in the back or one where the posterior palatal plane would converge to intersect the optic plane somewhere in the distance. This condition is thought to be brought on by the lack of posterior dental and skeletal growth that is often seen in patients with posterior deep bites. Patients with this condi-tion frequently have hyperactivity of the Masseter muscles that is common in TMJ, facial pain and headache patients. Patients with chronically enlarged palatine tonsils develop a protective swallowing pattern to avoid pain and gagging. This requires a complex system of muscle movement involving the tongue and buccal musculature. Over time, the activity of the buccal muscles inhibits growth of the mandibular rami, causing a superior posterior rotation of the palatal plane. Several points should be noted in most any anterior or posterior convergence is usually minimal and is only a few degrees (2-3° which fall within a standard deviation). The more extreme cases are quite easy to spot, and these are of patho-logical significance. Another consideration is that a vertical change in this relationship will create a corresponding change in the anterior skeletal vertical (proportion). This effect will change the perception of either a deep and or open bite that in fact may be neutral. Compensation by the clini-cian must be corrected in the ASV measurement based upon the rela-tive position of the ANS. Summary This extensively modified version of the Sassouni Cephalo-metric Analysis is very beneficial to the dentist treating functional orthodontics, airway obstructed and compromised patients. It is also useful in TMD and cran-iomandibular dysfunctional patients and those that have abnormal cervical alignment. Some practitioners even derive benefits from its application when deter-mining vertical in the edentulous and reconstruction patient. The Modified Sassouni Plus Analysis has been shown to be of great benefit to determine vertical proportion and growth potential of the young patient. The analysis has the ability to show incisor place-ment relative to opening and clos-ing trajectory used in Neuromuscu-lar Dentistry and where to place the mandible for functional advancement. Practitioners need a diagnostic cephalogram that is visual and descriptive of the skele-tal and dental malocclusion. This analysis provides many tools that will assist the clinician in making those decisions. www.orthodontics.com Fall 2021 27
Journal of the American Orthodontic Society Fall 2021: Page 27