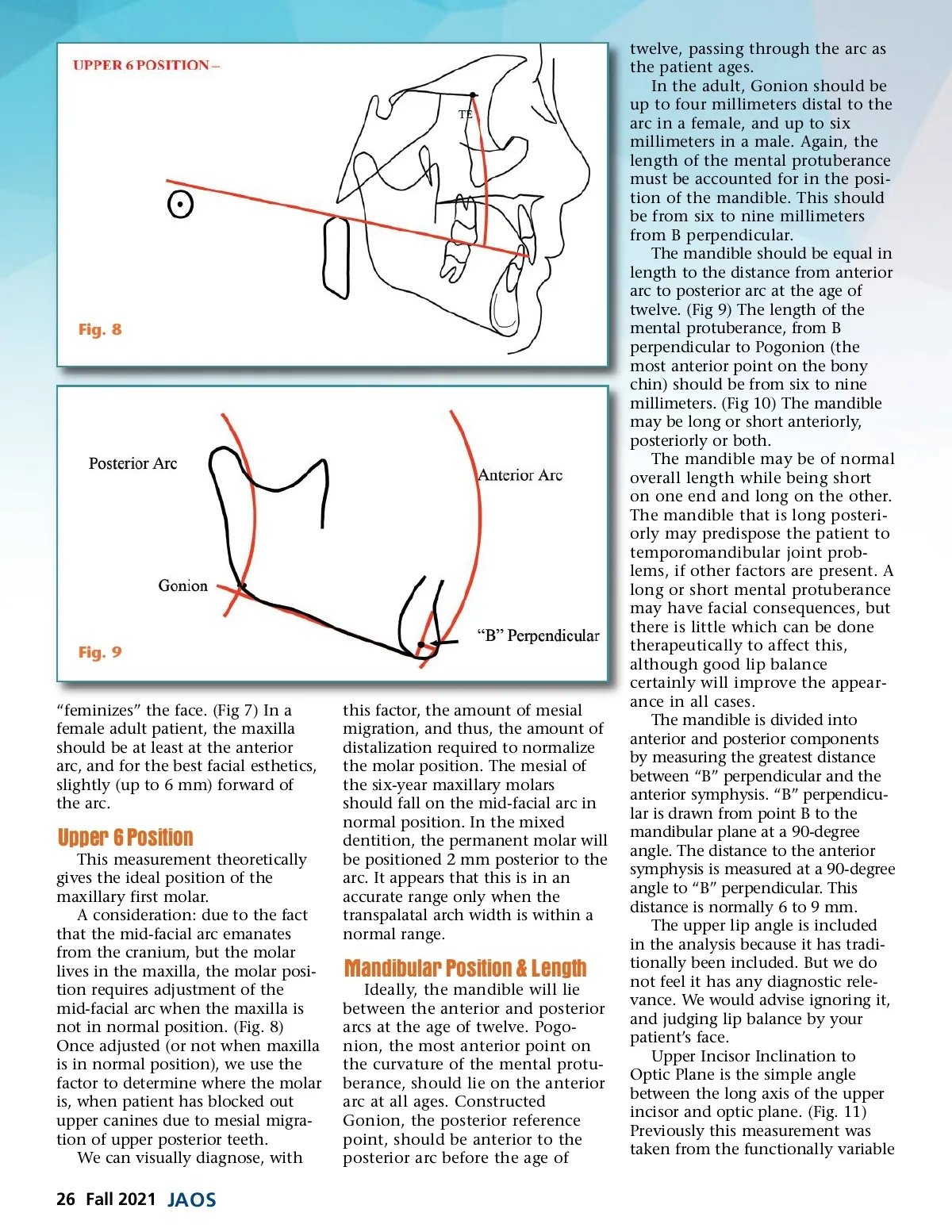
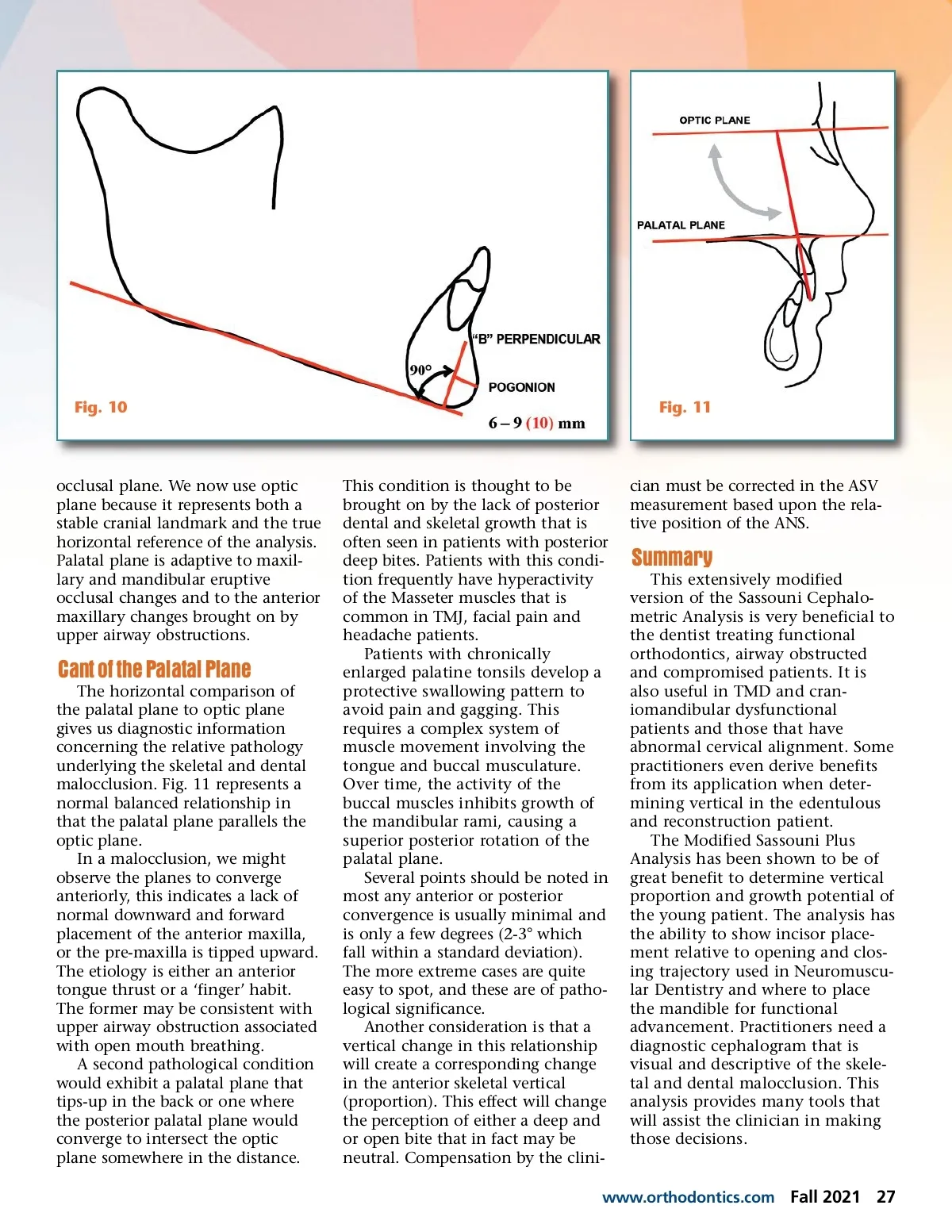
Fig. 8 Fig. 9 “feminizes” the face. (Fig 7) In a female adult patient, the maxilla should be at least at the anterior arc, and for the best facial esthetics, slightly (up to 6 mm) forward of the arc. Upper 6 Position This measurement theoretically gives the ideal position of the maxillary first molar. A consideration: due to the fact that the mid-facial arc emanates from the cranium, but the molar lives in the maxilla, the molar posi-tion requires adjustment of the mid-facial arc when the maxilla is not in normal position. (Fig. 8) Once adjusted (or not when maxilla is in normal position), we use the factor to determine where the molar is, when patient has blocked out upper canines due to mesial migra-tion of upper posterior teeth. We can visually diagnose, with this factor, the amount of mesial migration, and thus, the amount of distalization required to normalize the molar position. The mesial of the six-year maxillary molars should fall on the mid-facial arc in normal position. In the mixed dentition, the permanent molar will be positioned 2 mm posterior to the arc. It appears that this is in an accurate range only when the transpalatal arch width is within a normal range. Mandibular Position & Length Ideally, the mandible will lie between the anterior and posterior arcs at the age of twelve. Pogo-nion, the most anterior point on the curvature of the mental protu-berance, should lie on the anterior arc at all ages. Constructed Gonion, the posterior reference point, should be anterior to the posterior arc before the age of twelve, passing through the arc as the patient ages. In the adult, Gonion should be up to four millimeters distal to the arc in a female, and up to six millimeters in a male. Again, the length of the mental protuberance must be accounted for in the posi-tion of the mandible. This should be from six to nine millimeters from B perpendicular. The mandible should be equal in length to the distance from anterior arc to posterior arc at the age of twelve. (Fig 9) The length of the mental protuberance, from B perpendicular to Pogonion (the most anterior point on the bony chin) should be from six to nine millimeters. (Fig 10) The mandible may be long or short anteriorly, posteriorly or both. The mandible may be of normal overall length while being short on one end and long on the other. The mandible that is long posteri-orly may predispose the patient to temporomandibular joint prob-lems, if other factors are present. A long or short mental protuberance may have facial consequences, but there is little which can be done therapeutically to affect this, although good lip balance certainly will improve the appear-ance in all cases. The mandible is divided into anterior and posterior components by measuring the greatest distance between “B” perpendicular and the anterior symphysis. “B” perpendicu-lar is drawn from point B to the mandibular plane at a 90-degree angle. The distance to the anterior symphysis is measured at a 90-degree angle to “B” perpendicular. This distance is normally 6 to 9 mm. The upper lip angle is included in the analysis because it has tradi-tionally been included. But we do not feel it has any diagnostic rele-vance. We would advise ignoring it, and judging lip balance by your patient’s face. Upper Incisor Inclination to Optic Plane is the simple angle between the long axis of the upper incisor and optic plane. (Fig. 11) Previously this measurement was taken from the functionally variable 26 Fall 2021 JAOS
Journal of the American Orthodontic Society Fall 2021: Page 26