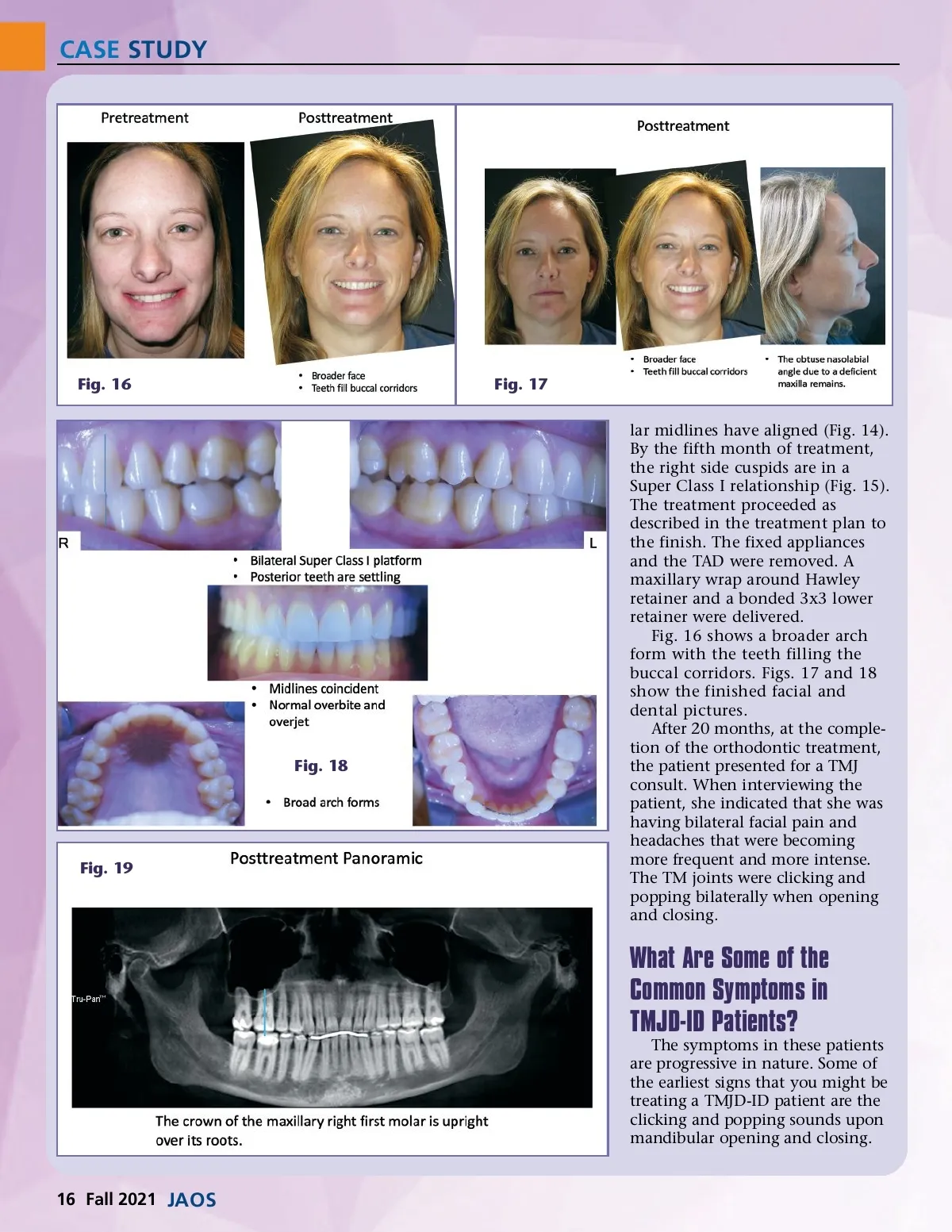
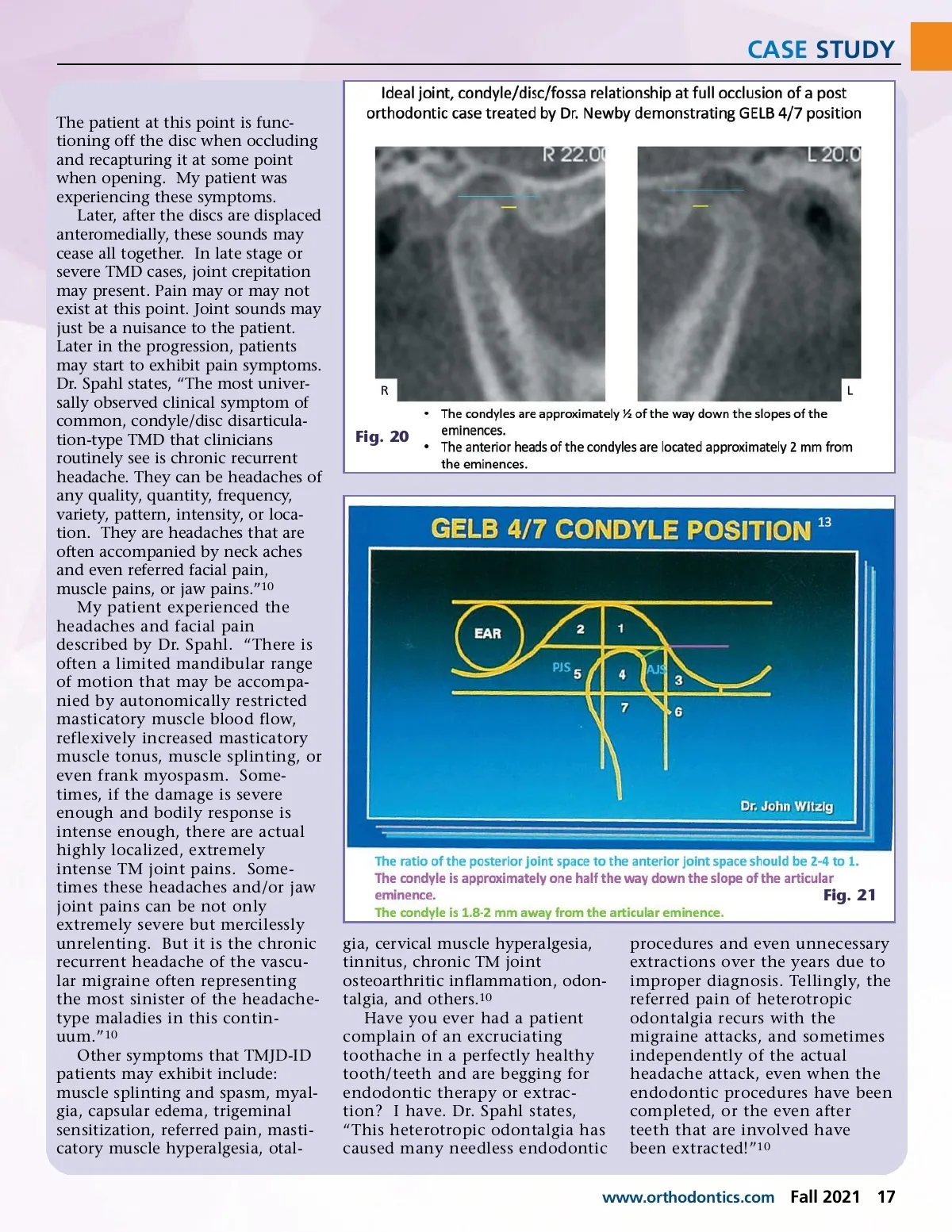
CASE STUDY The patient at this point is func-tioning off the disc when occluding and recapturing it at some point when opening. My patient was experiencing these symptoms. Later, after the discs are displaced anteromedially, these sounds may cease all together. In late stage or severe TMD cases, joint crepitation may present. Pain may or may not exist at this point. Joint sounds may just be a nuisance to the patient. Later in the progression, patients may start to exhibit pain symptoms. Dr. Spahl states, “The most univer-sally observed clinical symptom of common, condyle/disc disarticula-tion-type TMD that clinicians routinely see is chronic recurrent headache. They can be headaches of any quality, quantity, frequency, variety, pattern, intensity, or loca-tion. They are headaches that are often accompanied by neck aches and even referred facial pain, muscle pains, or jaw pains.” 10 My patient experienced the headaches and facial pain described by Dr. Spahl. “There is often a limited mandibular range of motion that may be accompa-nied by autonomically restricted masticatory muscle blood flow, reflexively increased masticatory muscle tonus, muscle splinting, or even frank myospasm. Some-times, if the damage is severe enough and bodily response is intense enough, there are actual highly localized, extremely intense TM joint pains. Some-times these headaches and/or jaw joint pains can be not only extremely severe but mercilessly unrelenting. But it is the chronic recurrent headache of the vascu-lar migraine often representing the most sinister of the headache-type maladies in this contin-uum.” 10 Other symptoms that TMJD-ID patients may exhibit include: muscle splinting and spasm, myal-gia, capsular edema, trigeminal sensitization, referred pain, masti-catory muscle hyperalgesia, otal-Fig. 20 Fig. 21 gia, cervical muscle hyperalgesia, tinnitus, chronic TM joint osteoarthritic inflammation, odon-talgia, and others. 10 Have you ever had a patient complain of an excruciating toothache in a perfectly healthy tooth/teeth and are begging for endodontic therapy or extrac-tion? I have. Dr. Spahl states, “This heterotropic odontalgia has caused many needless endodontic procedures and even unnecessary extractions over the years due to improper diagnosis. Tellingly, the referred pain of heterotropic odontalgia recurs with the migraine attacks, and sometimes independently of the actual headache attack, even when the endodontic procedures have been completed, or the even after teeth that are involved have been extracted!” 10 www.orthodontics.com Fall 2021 17
Journal of the American Orthodontic Society Fall 2021: Page 17