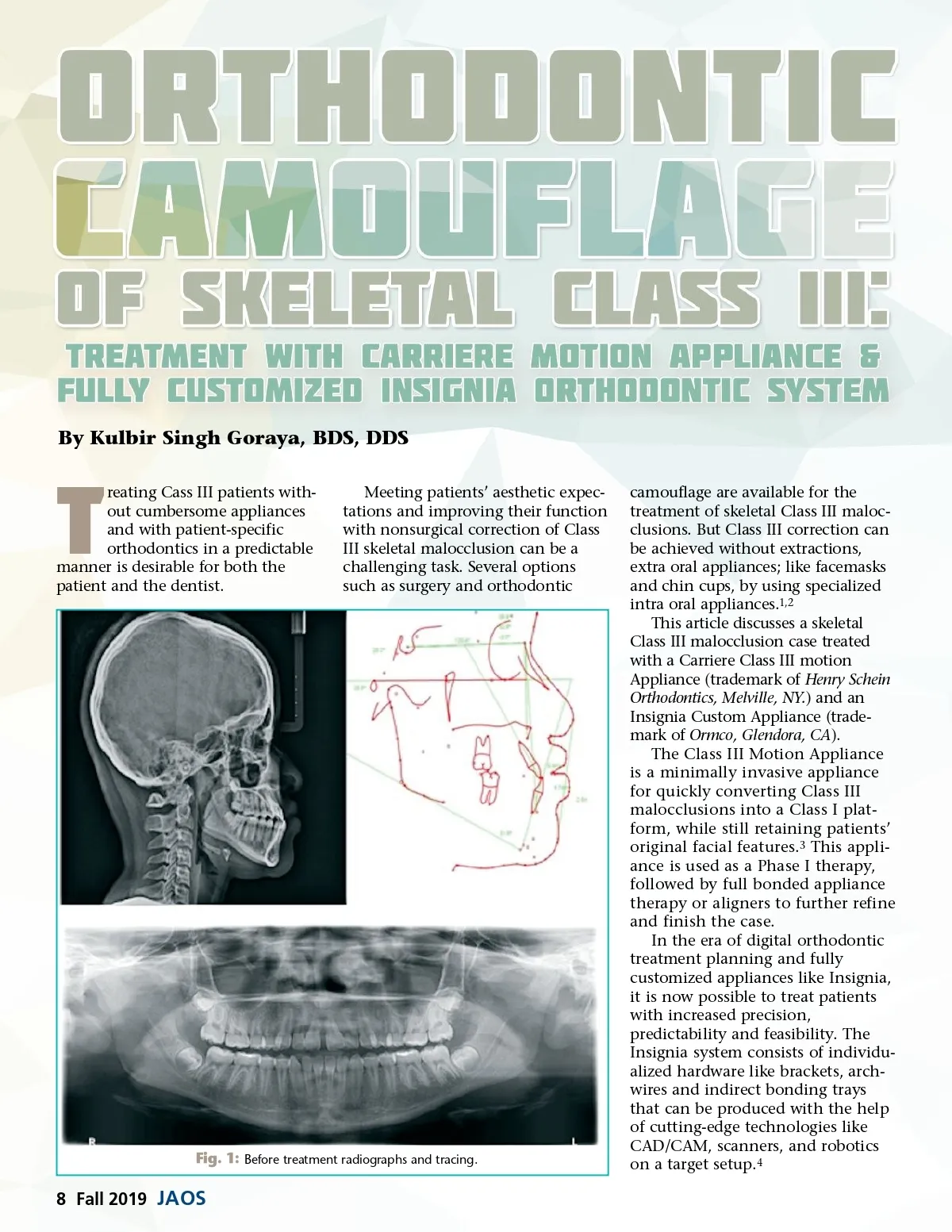
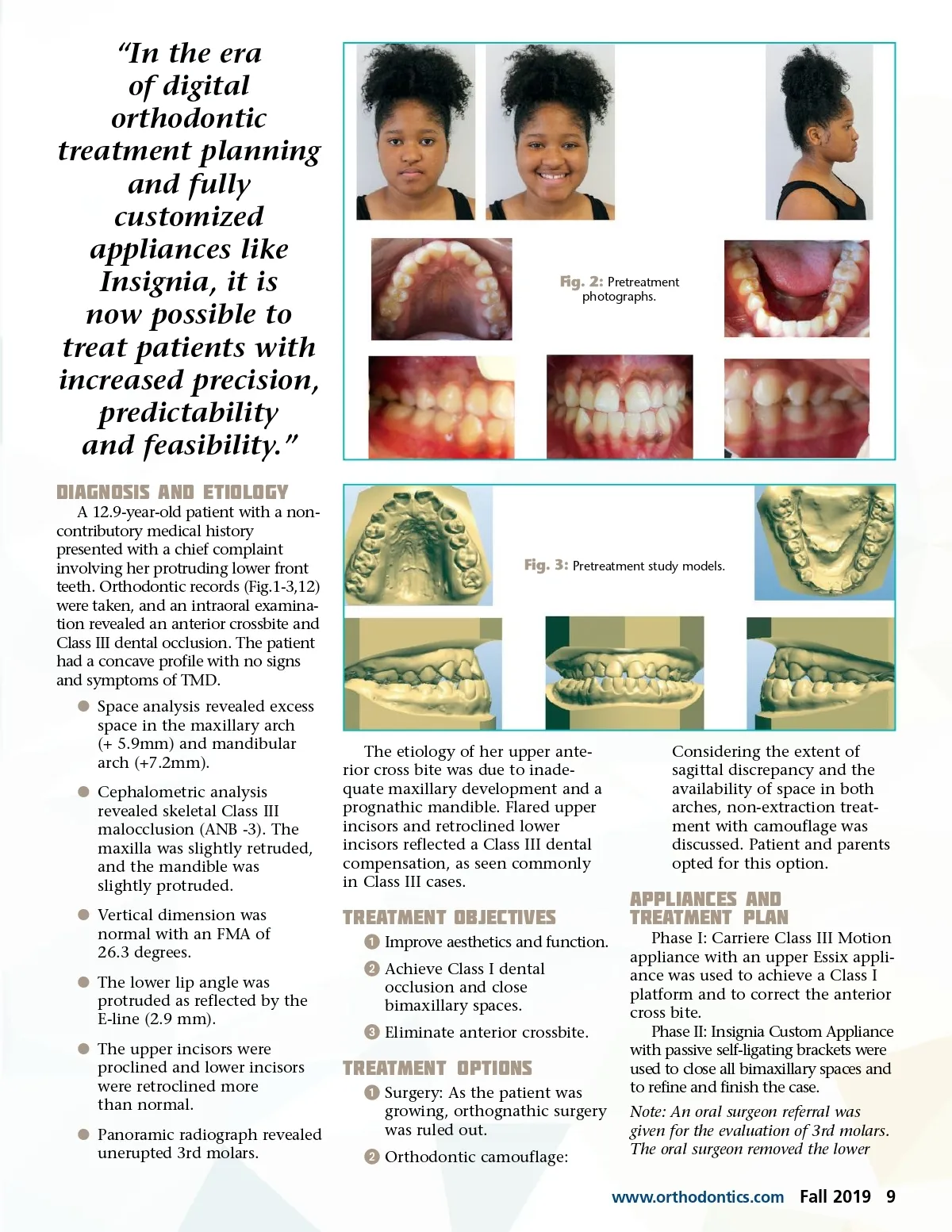
“In the era of digital orthodontic treatment planning and fully customized appliances like Insignia, it is now possible to treat patients with increased precision, predictability and feasibility.” Diagnosis and Etiology A 12.9-year-old patient with a non-contributory medical history presented with a chief complaint involving her protruding lower front teeth. Orthodontic records (Fig.1-3,12) were taken, and an intraoral examina-tion revealed an anterior crossbite and Class III dental occlusion. The patient had a concave profile with no signs and symptoms of TMD. b Space analysis revealed excess space in the maxillary arch (+ 5.9mm) and mandibular arch (+7.2mm). b Cephalometric analysis revealed skeletal Class III malocclusion (ANB -3). The maxilla was slightly retruded, and the mandible was slightly protruded. b Vertical dimension was normal with an FMA of 26.3 degrees. b The lower lip angle was protruded as reflected by the E-line (2.9 mm). b The upper incisors were proclined and lower incisors were retroclined more than normal. b Panoramic radiograph revealed unerupted 3rd molars. Fig. 2: Pretreatment photographs. Fig. 3: Pretreatment study models. The etiology of her upper ante-rior cross bite was due to inade-quate maxillary development and a prognathic mandible. Flared upper incisors and retroclined lower incisors reflected a Class III dental compensation, as seen commonly in Class III cases. Considering the extent of sagittal discrepancy and the availability of space in both arches, non-extraction treat-ment with camouflage was discussed. Patient and parents opted for this option. Treatment Objectives ᕡ Improve aesthetics and function. ᕢ Achieve Class I dental occlusion and close bimaxillary spaces. ᕣ Eliminate anterior crossbite. Appliances and Treatment Plan Phase I: Carriere Class III Motion appliance with an upper Essix appli-ance was used to achieve a Class I platform and to correct the anterior cross bite. Phase II: Insignia Custom Appliance with passive self-ligating brackets were used to close all bimaxillary spaces and to refine and finish the case. Note: An oral surgeon referral was given for the evaluation of 3rd molars. The oral surgeon removed the lower www.orthodontics.com Treatment Options ᕡ Surgery: As the patient was growing, orthognathic surgery was ruled out. ᕢ Orthodontic camouflage: Fall 2019 9
Journal of the American Orthodontic Society Fall 2019: Page 9