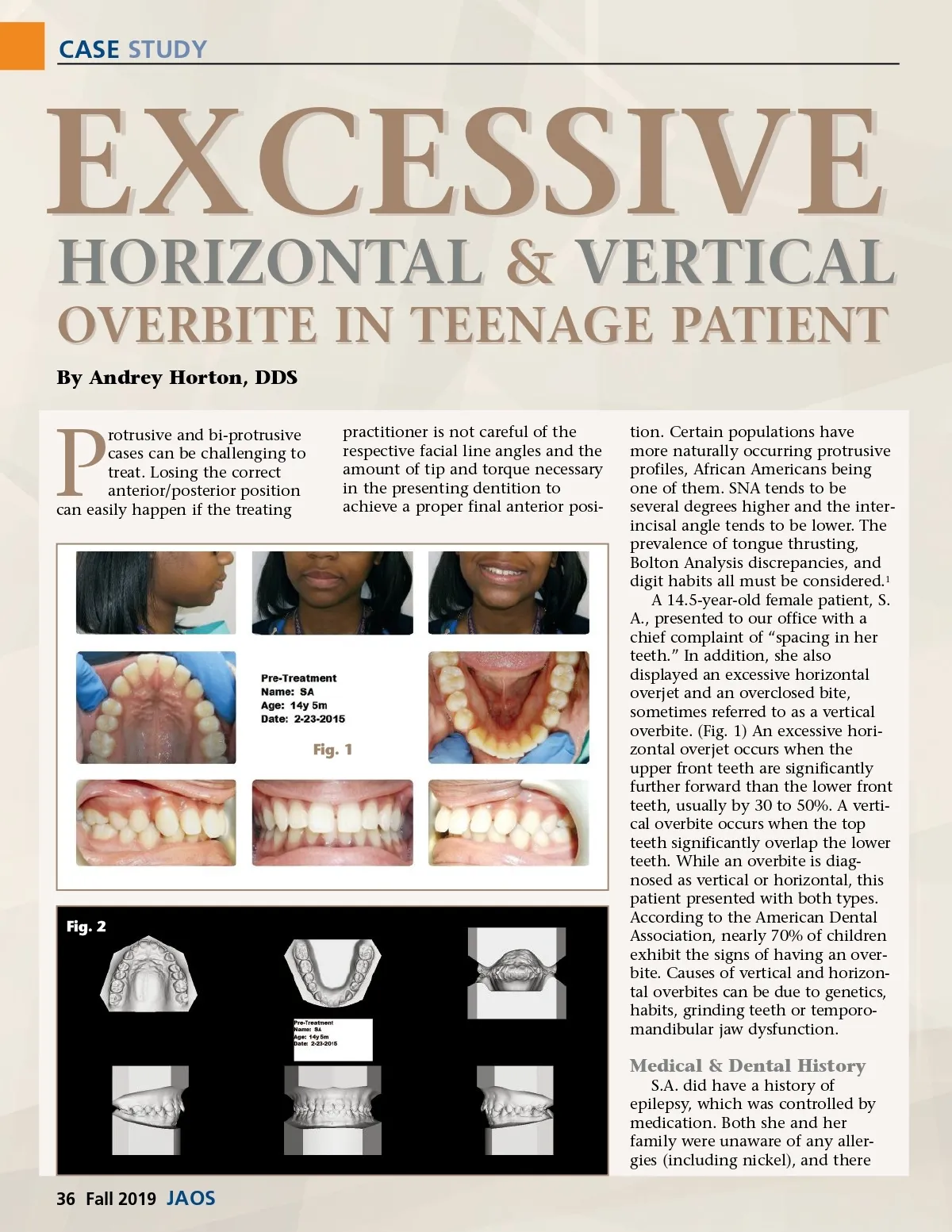
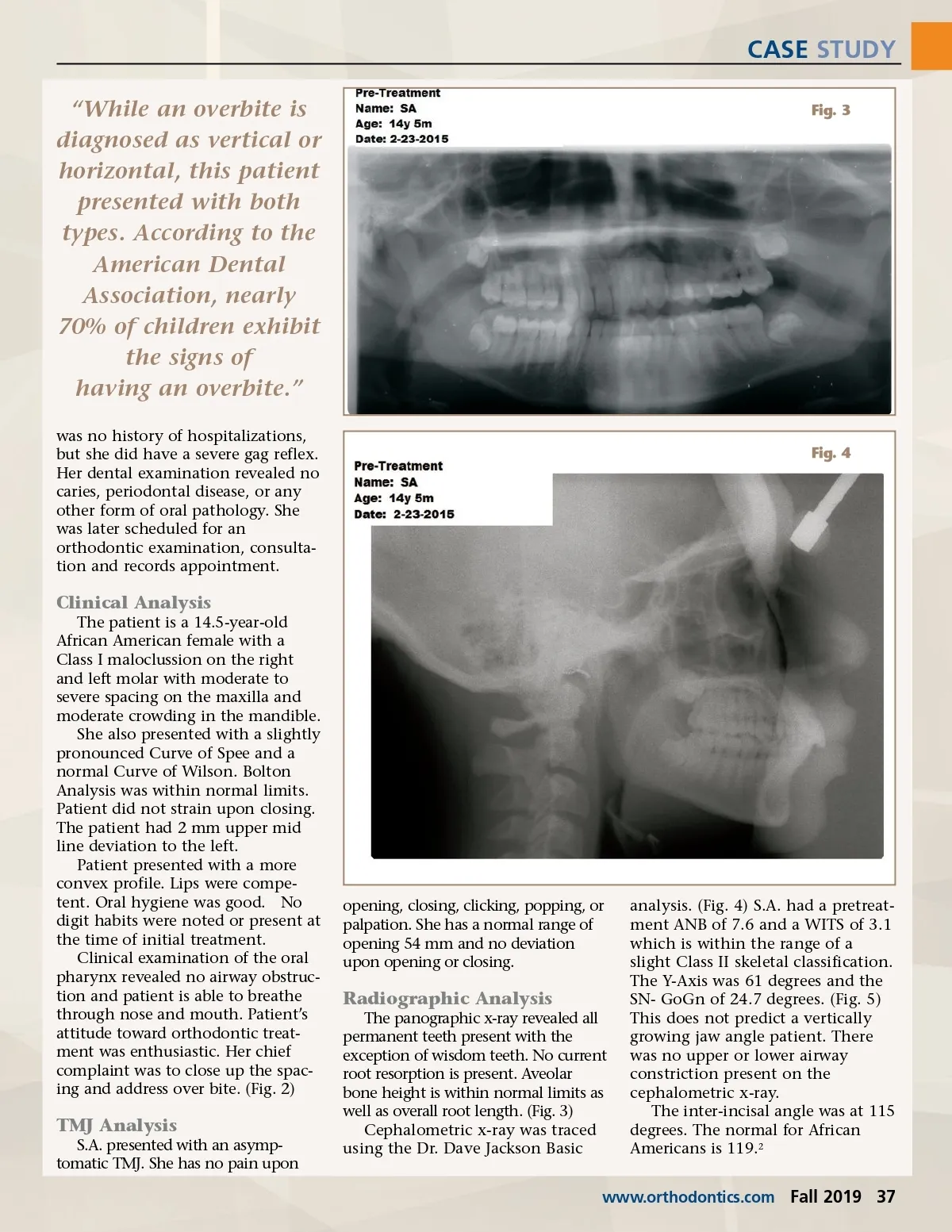
CASE STUDY EXCESSIVE HORIZONTAL & VERTICAL OVERBITE IN TEENAGE PATIENT By Andrey Horton, DDS P rotrusive and bi-protrusive cases can be challenging to treat. Losing the correct anterior/posterior position can easily happen if the treating practitioner is not careful of the respective facial line angles and the amount of tip and torque necessary in the presenting dentition to achieve a proper final anterior posi-Fig. 1 Fig. 2 tion. Certain populations have more naturally occurring protrusive profiles, African Americans being one of them. SNA tends to be several degrees higher and the inter-incisal angle tends to be lower. The prevalence of tongue thrusting, Bolton Analysis discrepancies, and digit habits all must be considered. 1 A 14.5-year-old female patient, S. A., presented to our office with a chief complaint of “spacing in her teeth.” In addition, she also displayed an excessive horizontal overjet and an overclosed bite, sometimes referred to as a vertical overbite. (Fig. 1) An excessive hori-zontal overjet occurs when the upper front teeth are significantly further forward than the lower front teeth, usually by 30 to 50%. A verti-cal overbite occurs when the top teeth significantly overlap the lower teeth. While an overbite is diag-nosed as vertical or horizontal, this patient presented with both types. According to the American Dental Association, nearly 70% of children exhibit the signs of having an over-bite. Causes of vertical and horizon-tal overbites can be due to genetics, habits, grinding teeth or temporo-mandibular jaw dysfunction. Medical & Dental History S.A. did have a history of epilepsy, which was controlled by medication. Both she and her family were unaware of any aller-gies (including nickel), and there 36 Fall 2019 JAOS
Journal of the American Orthodontic Society Fall 2019: Page 36