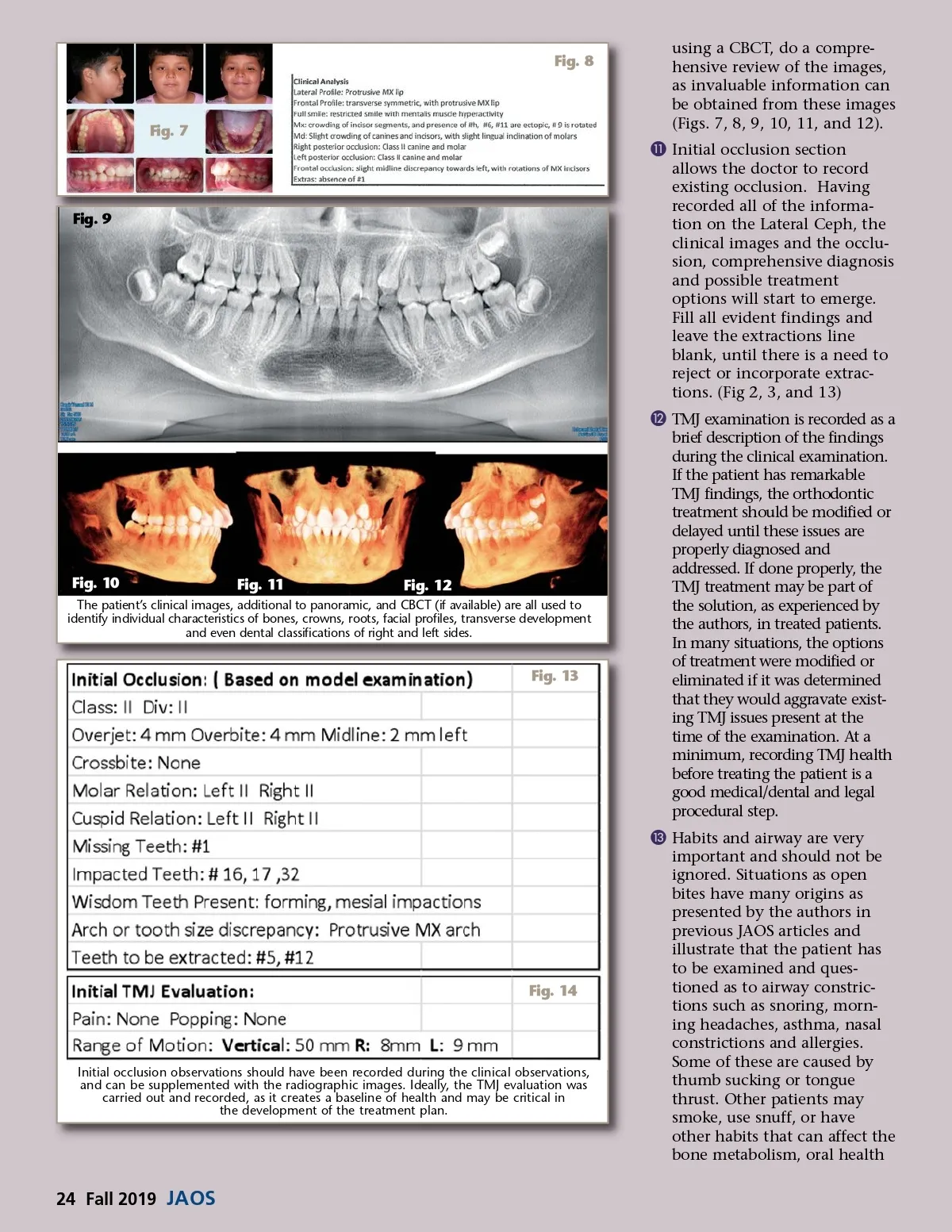
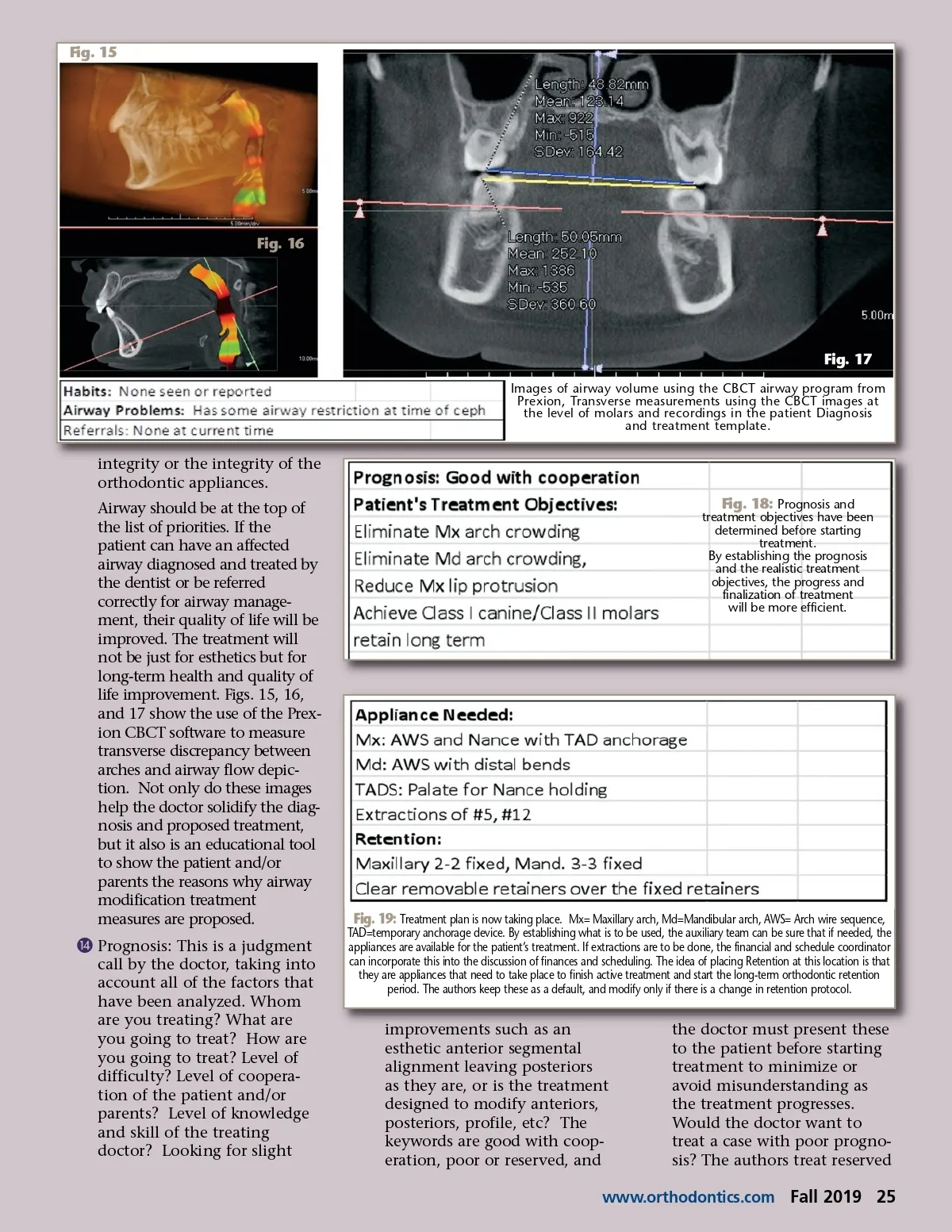
Fig. 15 Fig. 16 Fig. 17 Images of airway volume using the CBCT airway program from Prexion, Transverse measurements using the CBCT images at the level of molars and recordings in the patient Diagnosis and treatment template. integrity or the integrity of the orthodontic appliances. Airway should be at the top of the list of priorities. If the patient can have an affected airway diagnosed and treated by the dentist or be referred correctly for airway manage-ment, their quality of life will be improved. The treatment will not be just for esthetics but for long-term health and quality of life improvement. Figs. 15, 16, and 17 show the use of the Prex-ion CBCT software to measure transverse discrepancy between arches and airway flow depic-tion. Not only do these images help the doctor solidify the diag-nosis and proposed treatment, but it also is an educational tool to show the patient and/or parents the reasons why airway modification treatment measures are proposed. ƹ Prognosis: This is a judgment call by the doctor, taking into account all of the factors that have been analyzed. Whom are you treating? What are you going to treat? How are you going to treat? Level of difficulty? Level of coopera-tion of the patient and/or parents? Level of knowledge and skill of the treating doctor? Looking for slight Fig. 18: Prognosis and treatment objectives have been determined before starting treatment. By establishing the prognosis and the realistic treatment objectives, the progress and finalization of treatment will be more efficient. Fig. 19: Treatment plan is now taking place. Mx= Maxillary arch, Md=Mandibular arch, AWS= Arch wire sequence, TAD=temporary anchorage device. By establishing what is to be used, the auxiliary team can be sure that if needed, the appliances are available for the patient’s treatment. If extractions are to be done, the financial and schedule coordinator can incorporate this into the discussion of finances and scheduling. The idea of placing Retention at this location is that they are appliances that need to take place to finish active treatment and start the long-term orthodontic retention period. The authors keep these as a default, and modify only if there is a change in retention protocol. improvements such as an esthetic anterior segmental alignment leaving posteriors as they are, or is the treatment designed to modify anteriors, posteriors, profile, etc? The keywords are good with coop-eration, poor or reserved, and the doctor must present these to the patient before starting treatment to minimize or avoid misunderstanding as the treatment progresses. Would the doctor want to treat a case with poor progno-sis? The authors treat reserved www.orthodontics.com Fall 2019 25
Journal of the American Orthodontic Society Fall 2019: Page 25