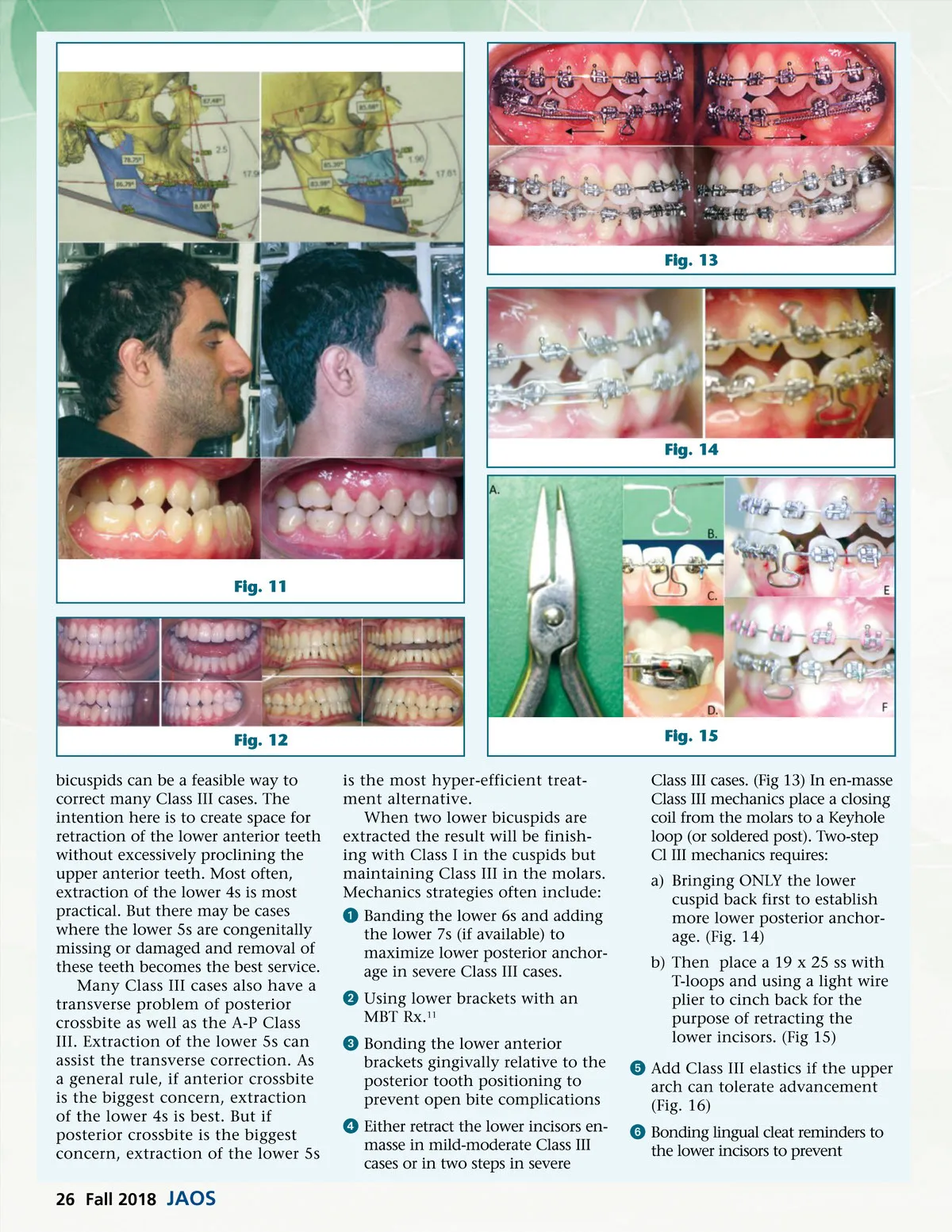
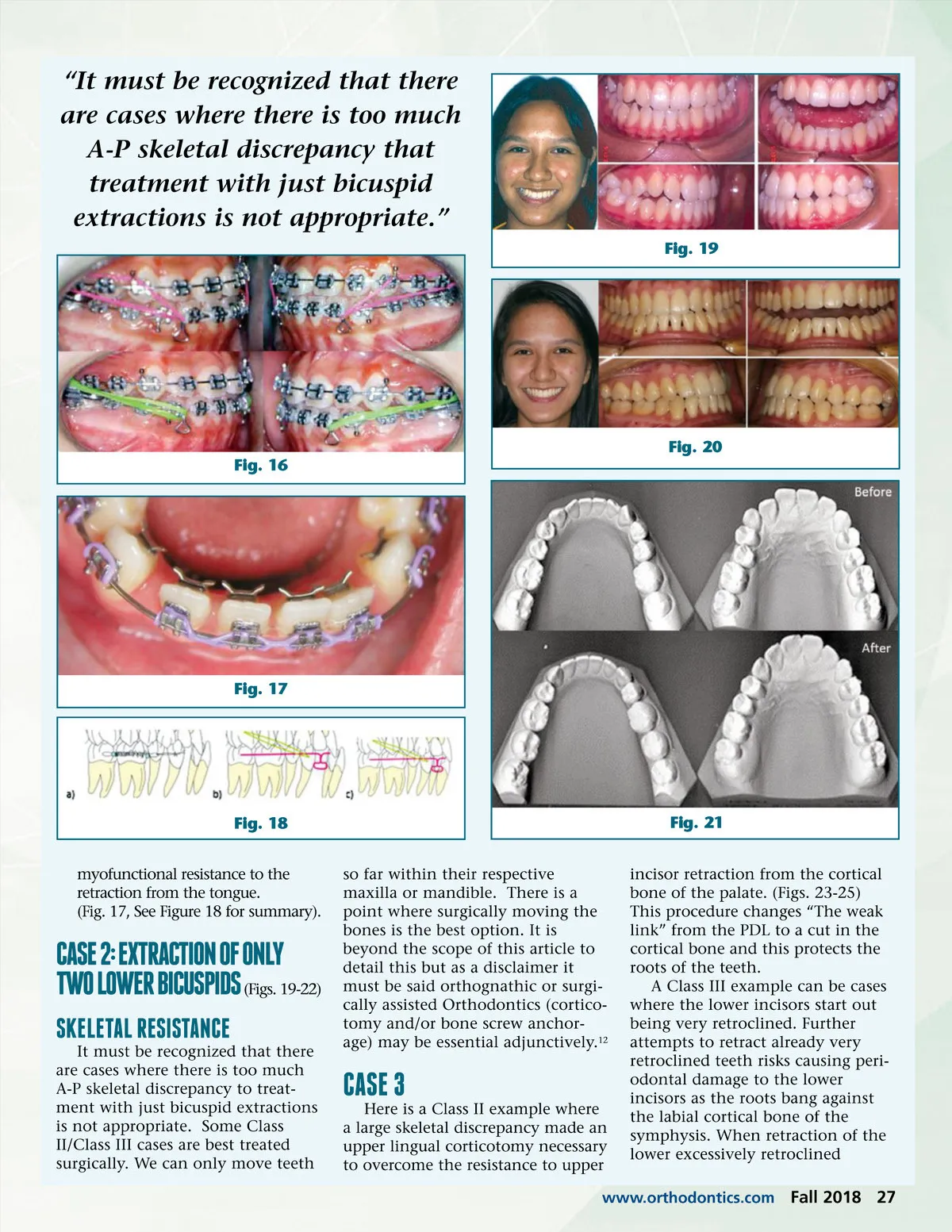
“It must be recognized that there are cases where there is too much A-P skeletal discrepancy that treatment with just bicuspid extractions is not appropriate.” Fig. 19 Fig. 20 Fig. 16 Fig. 17 Fig. 18 myofunctional resistance to the retraction from the tongue. (Fig. 17, See Figure 18 for summary). so far within their respective maxilla or mandible. There is a point where surgically moving the bones is the best option. It is beyond the scope of this article to detail this but as a disclaimer it must be said orthognathic or surgi-cally assisted Orthodontics (cortico-tomy and/or bone screw anchor-age) may be essential adjunctively. 12 Fig. 21 incisor retraction from the cortical bone of the palate. (Figs. 23-25) This procedure changes “The weak link” from the PDL to a cut in the cortical bone and this protects the roots of the teeth. A Class III example can be cases where the lower incisors start out being very retroclined. Further attempts to retract already very retroclined teeth risks causing peri-odontal damage to the lower incisors as the roots bang against the labial cortical bone of the symphysis. When retraction of the lower excessively retroclined CASE 2: EXTRACTION OF ONly TWO lOWER BICUSPIDS (Figs. 19-22) SkElETAl RESISTANCE It must be recognized that there are cases where there is too much A-P skeletal discrepancy to treat-ment with just bicuspid extractions is not appropriate. Some Class II/Class III cases are best treated surgically. We can only move teeth CASE 3 Here is a Class II example where a large skeletal discrepancy made an upper lingual corticotomy necessary to overcome the resistance to upper www.orthodontics.com Fall 2018 27
Journal of the American Orthodontic Society Fall 2018: Page 27