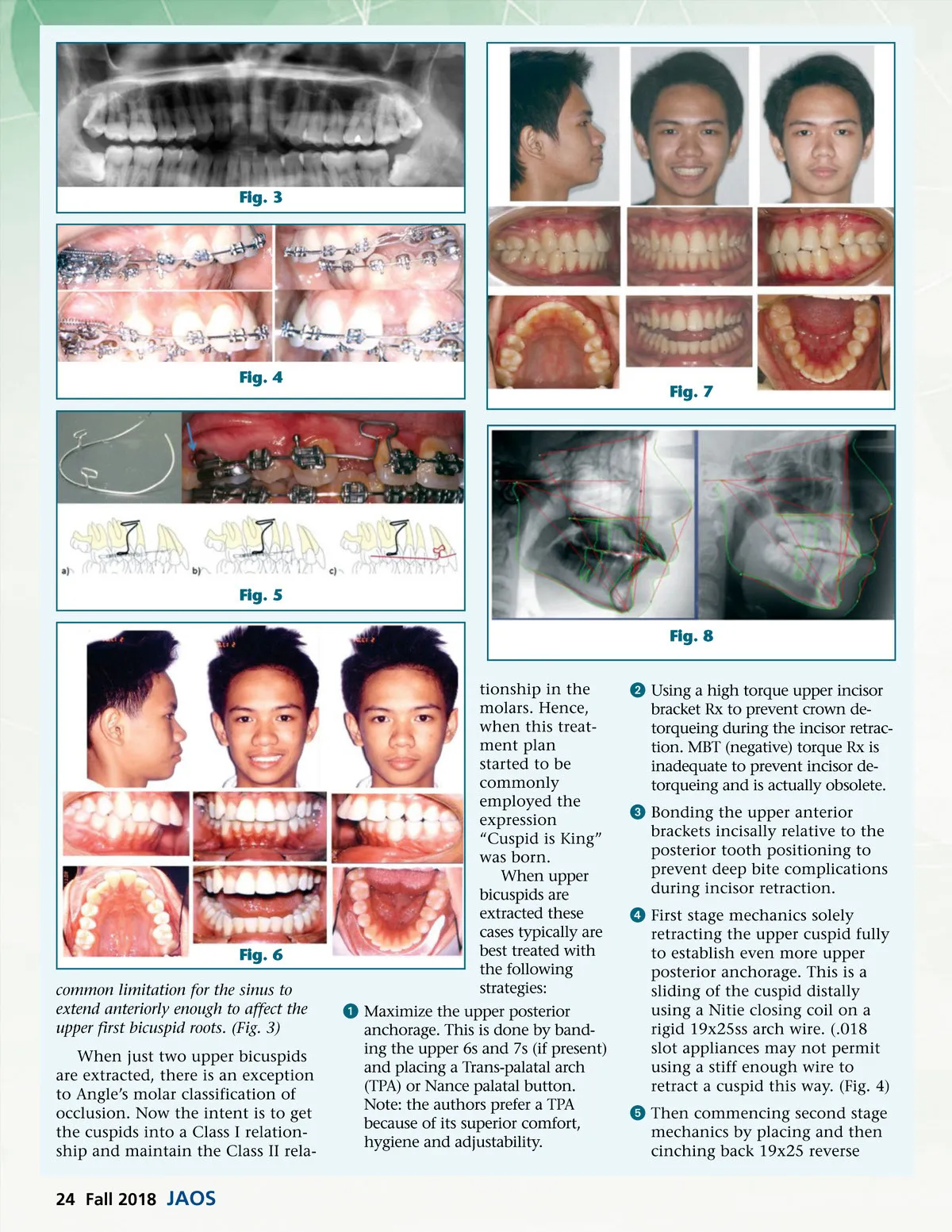
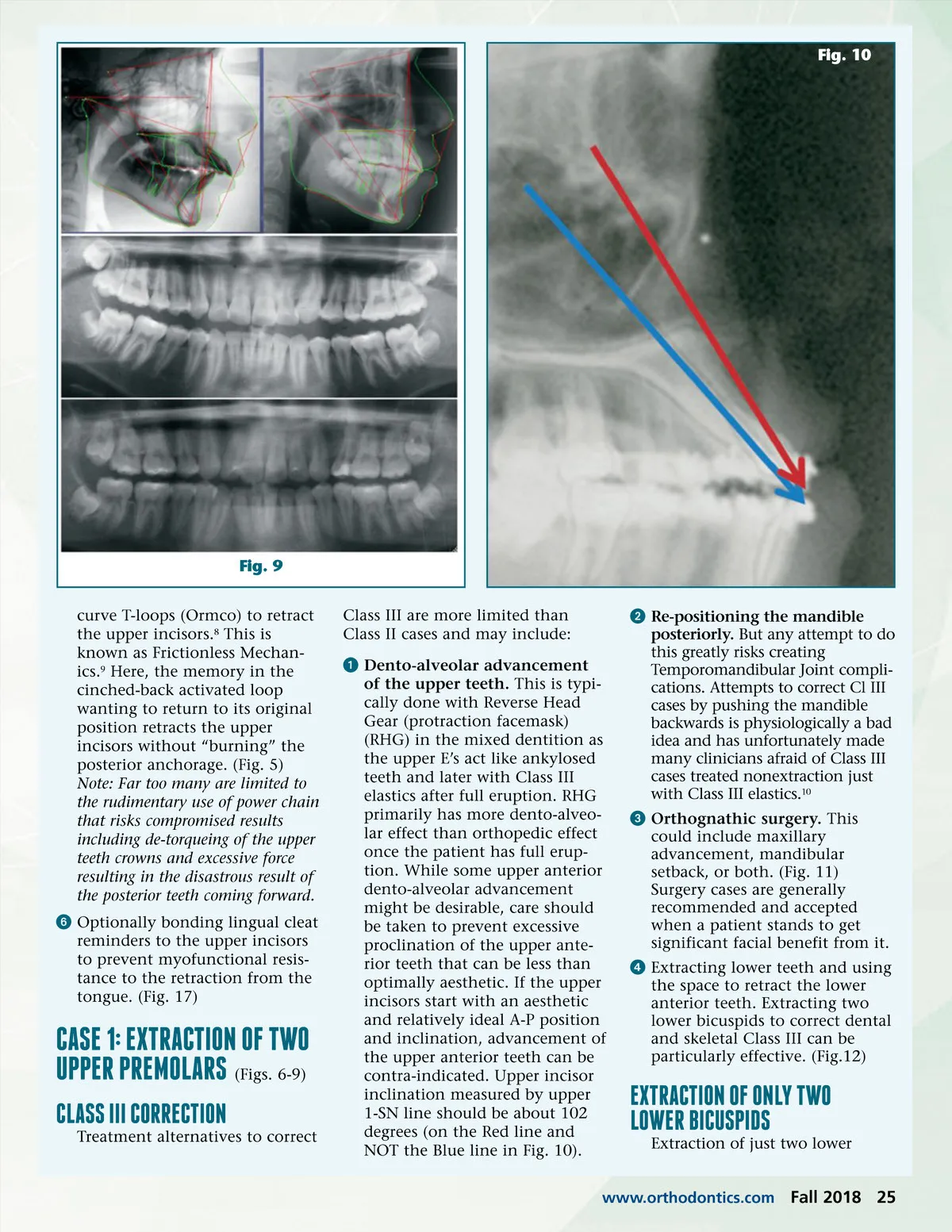
Fig. 10 Fig. 9 curve T-loops (Ormco) to retract the upper incisors. 8 This is known as Frictionless Mechan-ics. 9 Here, the memory in the cinched-back activated loop wanting to return to its original position retracts the upper incisors without “burning” the posterior anchorage. (Fig. 5) Note: Far too many are limited to the rudimentary use of power chain that risks compromised results including de-torqueing of the upper teeth crowns and excessive force resulting in the disastrous result of the posterior teeth coming forward. ᕦ Optionally bonding lingual cleat reminders to the upper incisors to prevent myofunctional resis-tance to the retraction from the tongue. (Fig. 17) Class III are more limited than Class II cases and may include: ᕡ Dento-alveolar advancement of the upper teeth. This is typi-cally done with Reverse Head Gear (protraction facemask) (RHG) in the mixed dentition as the upper E’s act like ankylosed teeth and later with Class III elastics after full eruption. RHG primarily has more dento-alveo-lar effect than orthopedic effect once the patient has full erup-tion. While some upper anterior dento-alveolar advancement might be desirable, care should be taken to prevent excessive proclination of the upper ante-rior teeth that can be less than optimally aesthetic. If the upper incisors start with an aesthetic and relatively ideal A-P position and inclination, advancement of the upper anterior teeth can be contra-indicated. Upper incisor inclination measured by upper 1-SN line should be about 102 degrees (on the Red line and NOT the Blue line in Fig. 10). ᕢ Re-positioning the mandible posteriorly. But any attempt to do this greatly risks creating Temporomandibular Joint compli-cations. Attempts to correct Cl III cases by pushing the mandible backwards is physiologically a bad idea and has unfortunately made many clinicians afraid of Class III cases treated nonextraction just with Class III elastics. 10 ᕣ Orthognathic surgery. This could include maxillary advancement, mandibular setback, or both. (Fig. 11) Surgery cases are generally recommended and accepted when a patient stands to get significant facial benefit from it. ᕤ Extracting lower teeth and using the space to retract the lower anterior teeth. Extracting two lower bicuspids to correct dental and skeletal Class III can be particularly effective. (Fig.12) CASE 1: EXTRACTION OF TWO UPPER PREMOlARS (Figs. 6-9) ClASS III CORRECTION Treatment alternatives to correct EXTRACTION OF ONly TWO lOWER BICUSPIDS Extraction of just two lower www.orthodontics.com Fall 2018 25
Journal of the American Orthodontic Society Fall 2018: Page 25