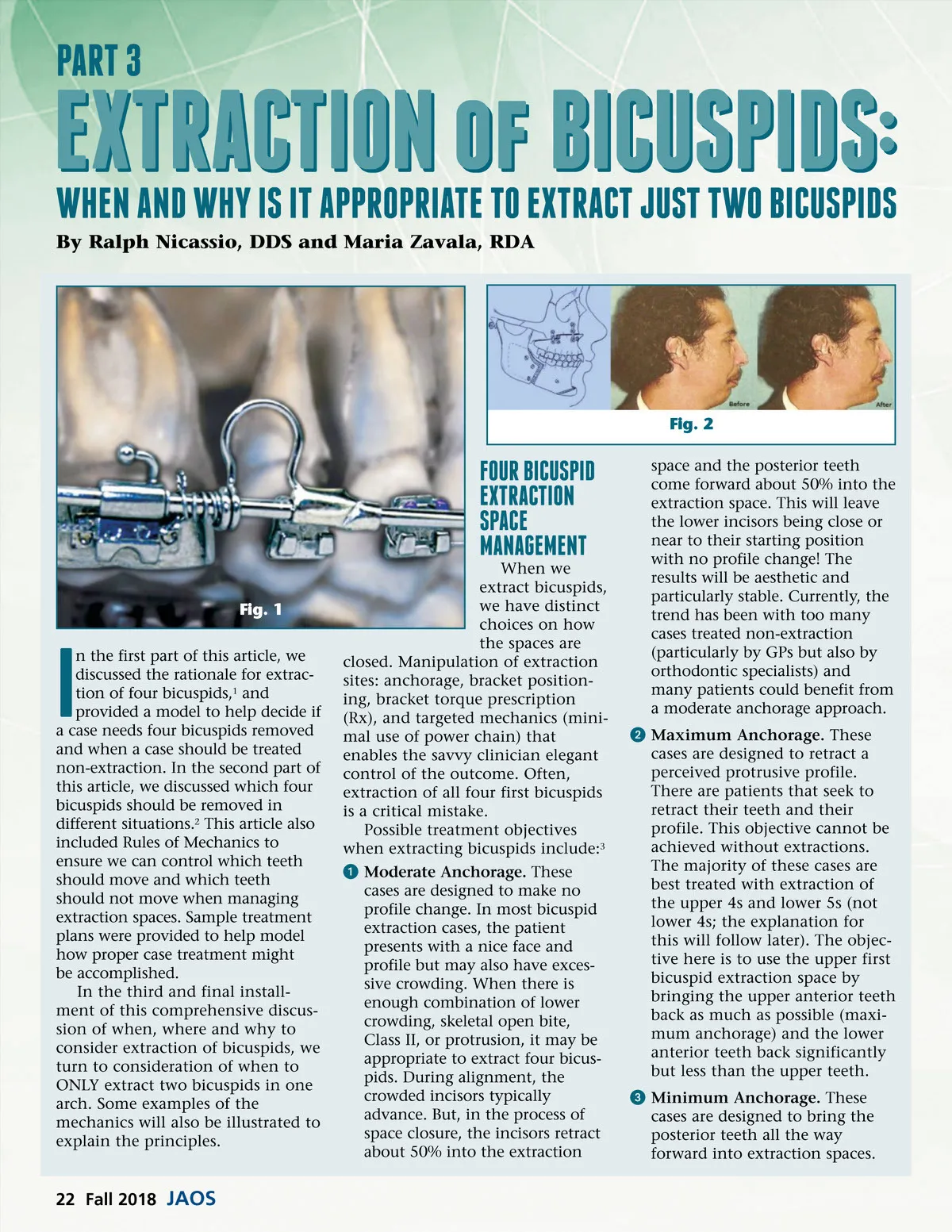
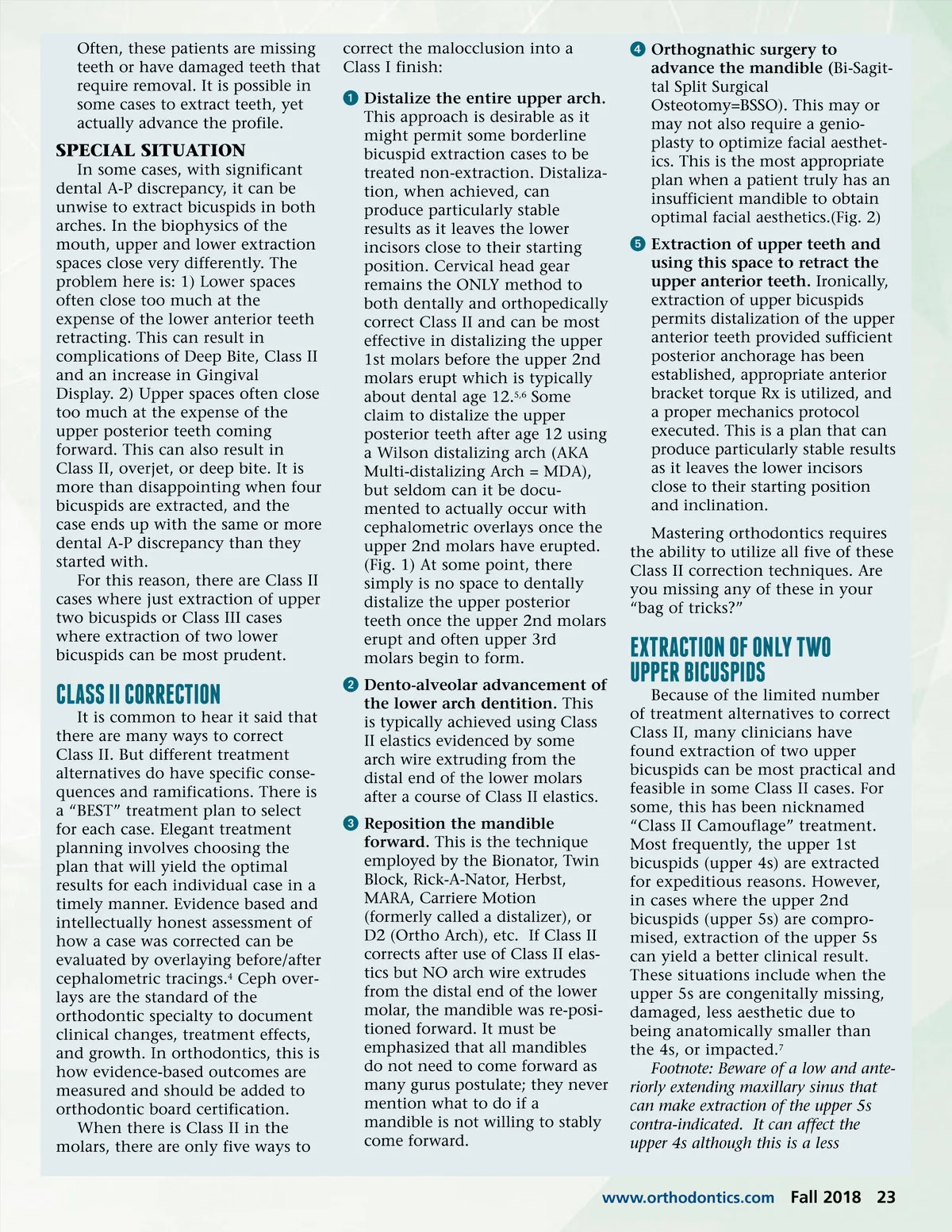
Often, these patients are missing teeth or have damaged teeth that require removal. It is possible in some cases to extract teeth, yet actually advance the profile. correct the malocclusion into a Class I finish: ᕡ Distalize the entire upper arch. This approach is desirable as it might permit some borderline bicuspid extraction cases to be treated non-extraction. Distaliza-tion, when achieved, can produce particularly stable results as it leaves the lower incisors close to their starting position. Cervical head gear remains the ONLY method to both dentally and orthopedically correct Class II and can be most effective in distalizing the upper 1st molars before the upper 2nd molars erupt which is typically about dental age 12. 5,6 Some claim to distalize the upper posterior teeth after age 12 using a Wilson distalizing arch (AKA Multi-distalizing Arch = MDA), but seldom can it be docu-mented to actually occur with cephalometric overlays once the upper 2nd molars have erupted. (Fig. 1) At some point, there simply is no space to dentally distalize the upper posterior teeth once the upper 2nd molars erupt and often upper 3rd molars begin to form. ᕢ Dento-alveolar advancement of the lower arch dentition. This is typically achieved using Class II elastics evidenced by some arch wire extruding from the distal end of the lower molars after a course of Class II elastics. ᕣ Reposition the mandible forward. This is the technique employed by the Bionator, Twin Block, Rick-A-Nator, Herbst, MARA, Carriere Motion (formerly called a distalizer), or D2 (Ortho Arch), etc. If Class II corrects after use of Class II elas-tics but NO arch wire extrudes from the distal end of the lower molar, the mandible was re-posi-tioned forward. It must be emphasized that all mandibles do not need to come forward as many gurus postulate; they never mention what to do if a mandible is not willing to stably come forward. SPECIAL SITUATION In some cases, with significant dental A-P discrepancy, it can be unwise to extract bicuspids in both arches. In the biophysics of the mouth, upper and lower extraction spaces close very differently. The problem here is: 1) Lower spaces often close too much at the expense of the lower anterior teeth retracting. This can result in complications of Deep Bite, Class II and an increase in Gingival Display. 2) Upper spaces often close too much at the expense of the upper posterior teeth coming forward. This can also result in Class II, overjet, or deep bite. It is more than disappointing when four bicuspids are extracted, and the case ends up with the same or more dental A-P discrepancy than they started with. For this reason, there are Class II cases where just extraction of upper two bicuspids or Class III cases where extraction of two lower bicuspids can be most prudent. ᕤ Orthognathic surgery to advance the mandible ( Bi-Sagit-tal Split Surgical Osteotomy=BSSO). This may or may not also require a genio-plasty to optimize facial aesthet-ics. This is the most appropriate plan when a patient truly has an insufficient mandible to obtain optimal facial aesthetics.(Fig. 2) ᕥ Extraction of upper teeth and using this space to retract the upper anterior teeth. Ironically, extraction of upper bicuspids permits distalization of the upper anterior teeth provided sufficient posterior anchorage has been established, appropriate anterior bracket torque Rx is utilized, and a proper mechanics protocol executed. This is a plan that can produce particularly stable results as it leaves the lower incisors close to their starting position and inclination. Mastering orthodontics requires the ability to utilize all five of these Class II correction techniques. Are you missing any of these in your “bag of tricks?” ClASS II CORRECTION It is common to hear it said that there are many ways to correct Class II. But different treatment alternatives do have specific conse-quences and ramifications. There is a “BEST” treatment plan to select for each case. Elegant treatment planning involves choosing the plan that will yield the optimal results for each individual case in a timely manner. Evidence based and intellectually honest assessment of how a case was corrected can be evaluated by overlaying before/after cephalometric tracings. 4 Ceph over-lays are the standard of the orthodontic specialty to document clinical changes, treatment effects, and growth. In orthodontics, this is how evidence-based outcomes are measured and should be added to orthodontic board certification. When there is Class II in the molars, there are only five ways to EXTRACTION OF ONly TWO UPPER BICUSPIDS Because of the limited number of treatment alternatives to correct Class II, many clinicians have found extraction of two upper bicuspids can be most practical and feasible in some Class II cases. For some, this has been nicknamed “Class II Camouflage” treatment. Most frequently, the upper 1st bicuspids (upper 4s) are extracted for expeditious reasons. However, in cases where the upper 2nd bicuspids (upper 5s) are compro-mised, extraction of the upper 5s can yield a better clinical result. These situations include when the upper 5s are congenitally missing, damaged, less aesthetic due to being anatomically smaller than the 4s, or impacted. 7 Footnote: Beware of a low and ante-riorly extending maxillary sinus that can make extraction of the upper 5s contra-indicated. It can affect the upper 4s although this is a less www.orthodontics.com Fall 2018 23
Journal of the American Orthodontic Society Fall 2018: Page 23