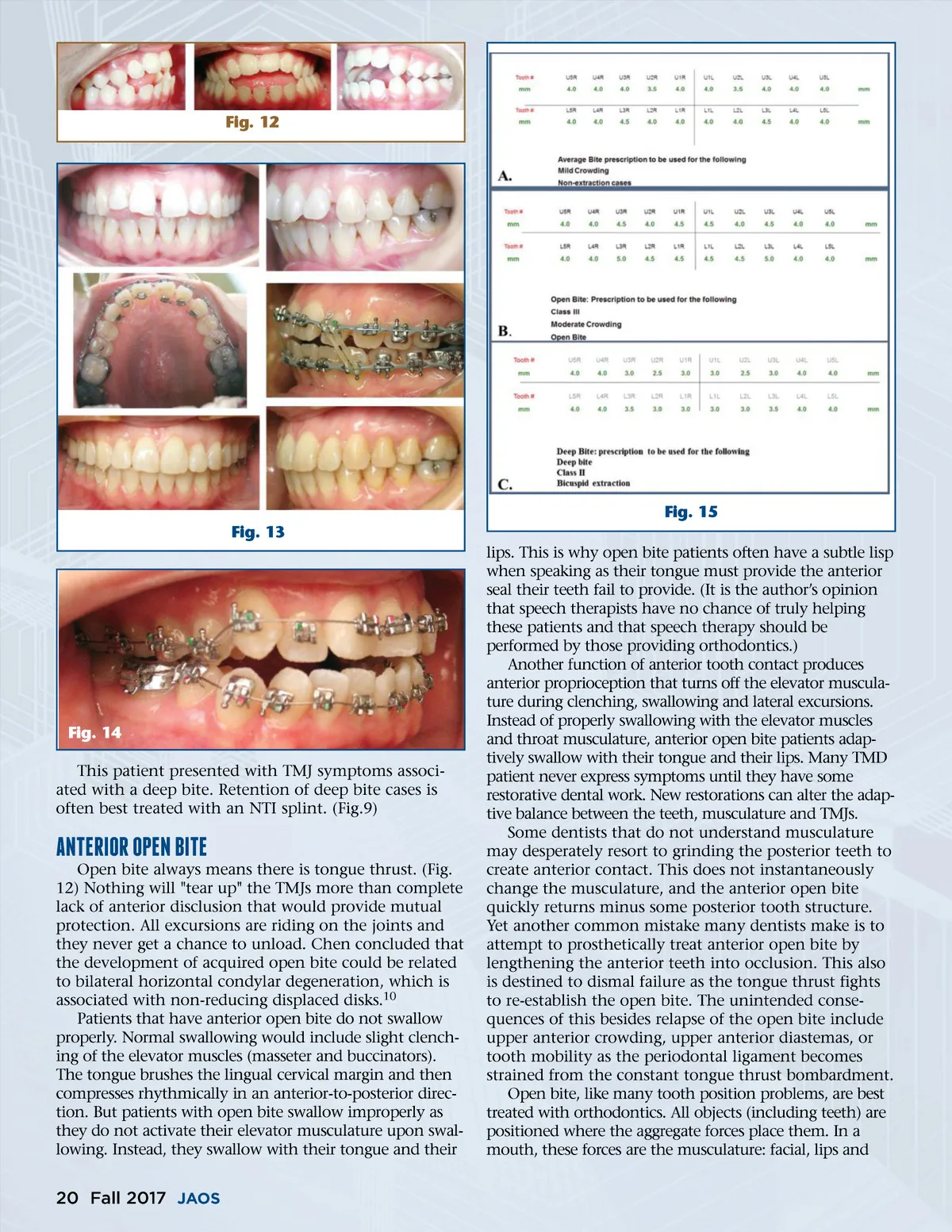
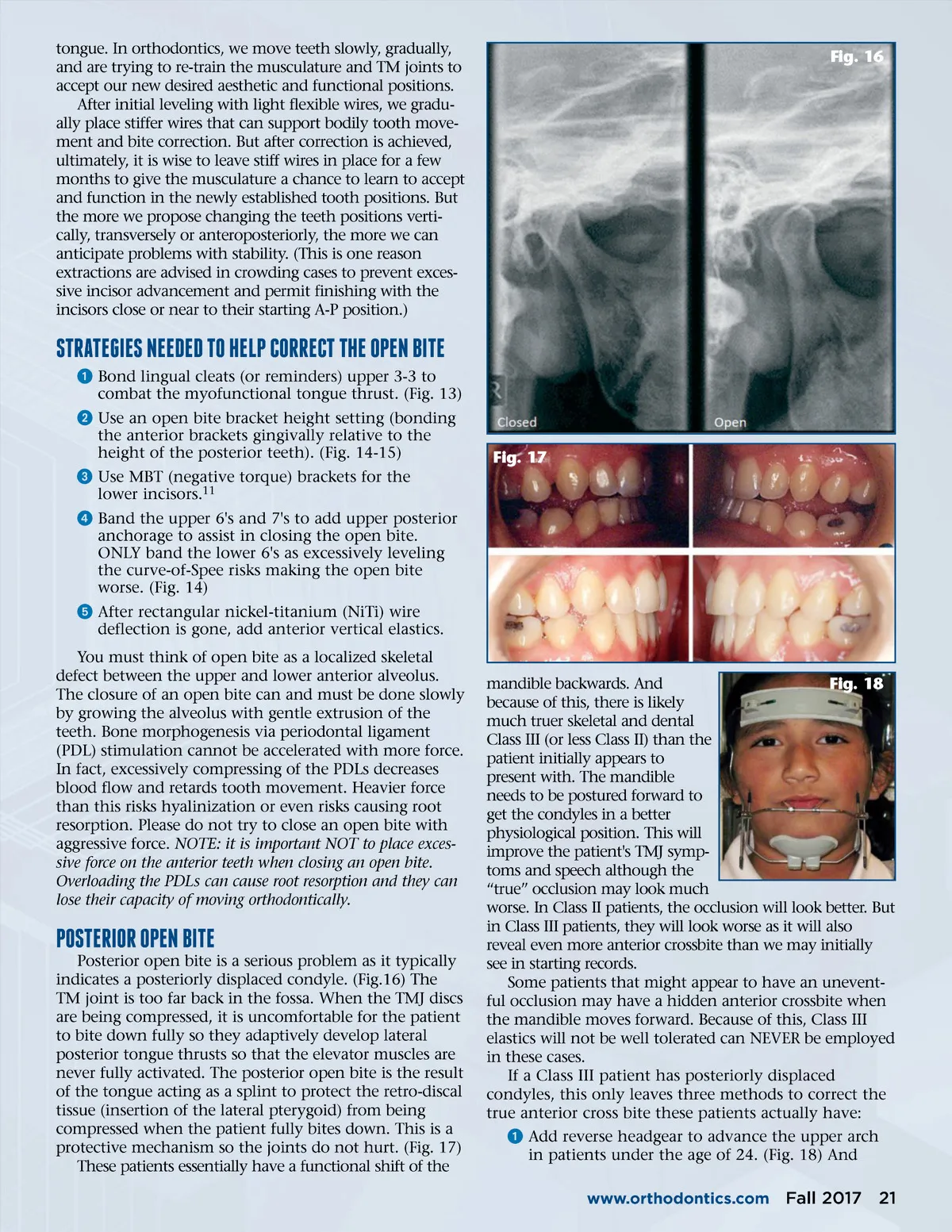
tongue. In orthodontics, we move teeth slowly, gradually, and are trying to re-train the musculature and TM joints to accept our new desired aesthetic and functional positions. After initial leveling with light flexible wires, we gradu-ally place stiffer wires that can support bodily tooth move-ment and bite correction. But after correction is achieved, ultimately, it is wise to leave stiff wires in place for a few months to give the musculature a chance to learn to accept and function in the newly established tooth positions. But the more we propose changing the teeth positions verti-cally, transversely or anteroposteriorly, the more we can anticipate problems with stability. (This is one reason extractions are advised in crowding cases to prevent exces-sive incisor advancement and permit finishing with the incisors close or near to their starting A-P position.) Fig. 16 sTRATEgIEs NEEDED TO hElp CORRECT ThE OpEN BITE ᕡ Bond lingual cleats (or reminders) upper 3-3 to combat the myofunctional tongue thrust. (Fig. 13) ᕢ Use an open bite bracket height setting (bonding the anterior brackets gingivally relative to the height of the posterior teeth). (Fig. 14-15) ᕣ Use MBT (negative torque) brackets for the lower incisors. 11 ᕤ Band the upper 6's and 7's to add upper posterior anchorage to assist in closing the open bite. ONLY band the lower 6's as excessively leveling the curve-of-Spee risks making the open bite worse. (Fig. 14) ᕥ After rectangular nickel-titanium (NiTi) wire deflection is gone, add anterior vertical elastics. You must think of open bite as a localized skeletal defect between the upper and lower anterior alveolus. The closure of an open bite can and must be done slowly by growing the alveolus with gentle extrusion of the teeth. Bone morphogenesis via periodontal ligament (PDL) stimulation cannot be accelerated with more force. In fact, excessively compressing of the PDLs decreases blood flow and retards tooth movement. Heavier force than this risks hyalinization or even risks causing root resorption. Please do not try to close an open bite with aggressive force. NOTE: it is important NOT to place exces-sive force on the anterior teeth when closing an open bite. Overloading the PDLs can cause root resorption and they can lose their capacity of moving orthodontically. Fig. 17 pOsTERIOR OpEN BITE Posterior open bite is a serious problem as it typically indicates a posteriorly displaced condyle. (Fig.16) The TM joint is too far back in the fossa. When the TMJ discs are being compressed, it is uncomfortable for the patient to bite down fully so they adaptively develop lateral posterior tongue thrusts so that the elevator muscles are never fully activated. The posterior open bite is the result of the tongue acting as a splint to protect the retro-discal tissue (insertion of the lateral pterygoid) from being compressed when the patient fully bites down. This is a protective mechanism so the joints do not hurt. (Fig. 17) These patients essentially have a functional shift of the mandible backwards. And Fig. 18 because of this, there is likely much truer skeletal and dental Class III (or less Class II) than the patient initially appears to present with. The mandible needs to be postured forward to get the condyles in a better physiological position. This will improve the patient's TMJ symp-toms and speech although the “true” occlusion may look much worse. In Class II patients, the occlusion will look better. But in Class III patients, they will look worse as it will also reveal even more anterior crossbite than we may initially see in starting records. Some patients that might appear to have an unevent-ful occlusion may have a hidden anterior crossbite when the mandible moves forward. Because of this, Class III elastics will not be well tolerated can NEVER be employed in these cases. If a Class III patient has posteriorly displaced condyles, this only leaves three methods to correct the true anterior cross bite these patients actually have: ᕡ Add reverse headgear to advance the upper arch in patients under the age of 24. (Fig. 18) And www.orthodontics.com Fall 2017 21
Journal of the American Orthodontic Society Fall 2017: Page 21