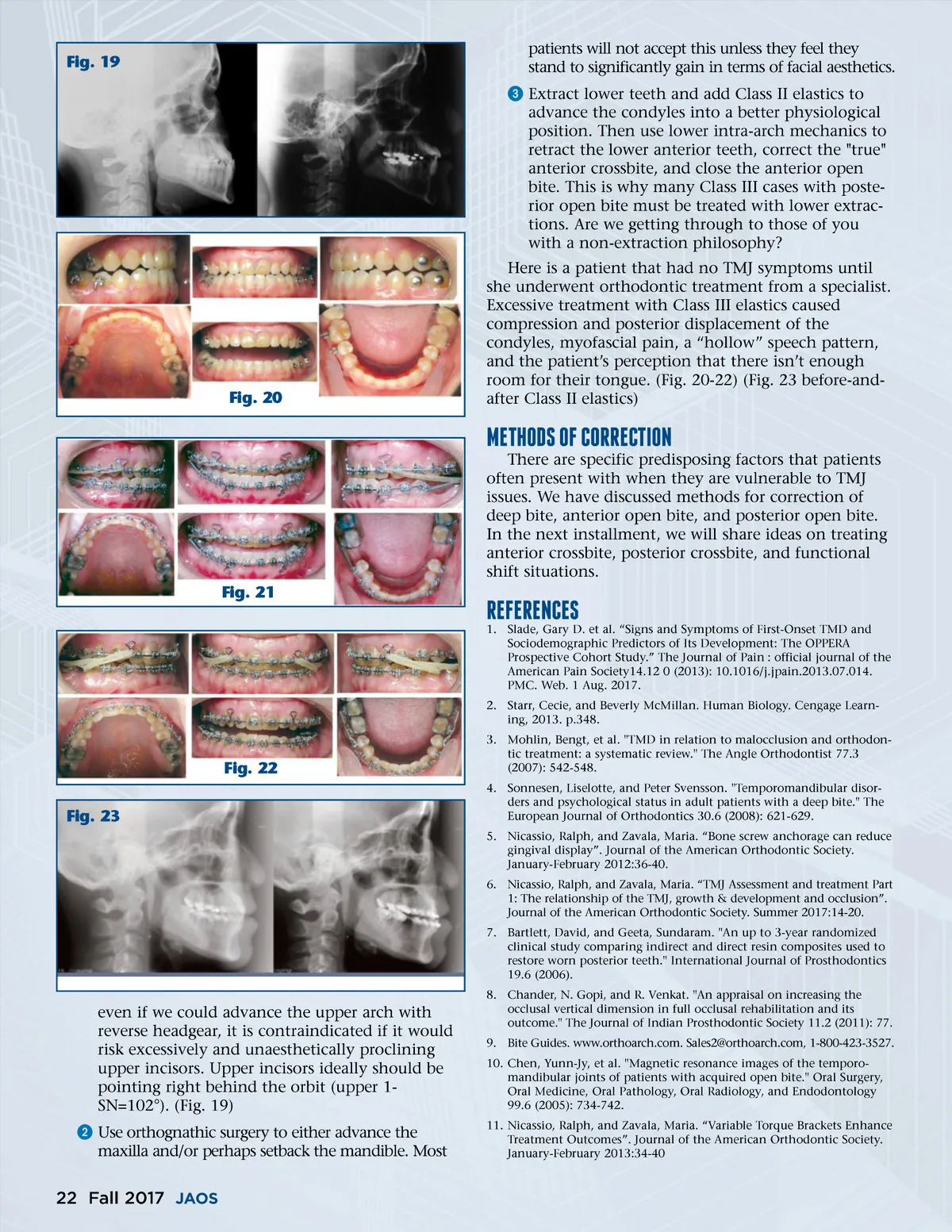
Fig. 19 patients will not accept this unless they feel they stand to significantly gain in terms of facial aesthetics. ᕣ Extract lower teeth and add Class II elastics to advance the condyles into a better physiological position. Then use lower intra-arch mechanics to retract the lower anterior teeth, correct the "true" anterior crossbite, and close the anterior open bite. This is why many Class III cases with poste-rior open bite must be treated with lower extrac-tions. Are we getting through to those of you with a non-extraction philosophy? Here is a patient that had no TMJ symptoms until she underwent orthodontic treatment from a specialist. Excessive treatment with Class III elastics caused compression and posterior displacement of the condyles, myofascial pain, a “hollow” speech pattern, and the patient’s perception that there isn’t enough room for their tongue. (Fig. 20-22) (Fig. 23 before-and-after Class II elastics) Fig. 20 METhODs Of CORRECTION There are specific predisposing factors that patients often present with when they are vulnerable to TMJ issues. We have discussed methods for correction of deep bite, anterior open bite, and posterior open bite. In the next installment, we will share ideas on treating anterior crossbite, posterior crossbite, and functional shift situations. Fig. 21 REfERENCEs 1. Slade, Gary D. et al. “Signs and Symptoms of First-Onset TMD and Sociodemographic Predictors of Its Development: The OPPERA Prospective Cohort Study.” The Journal of Pain : official journal of the American Pain Society14.12 0 (2013): 10.1016/j.jpain.2013.07.014. PMC. Web. 1 Aug. 2017. 2. Starr, Cecie, and Beverly McMillan. Human Biology. Cengage Learn-ing, 2013. p.348. 3. Mohlin, Bengt, et al. "TMD in relation to malocclusion and orthodon-tic treatment: a systematic review." The Angle Orthodontist 77.3 (2007): 542-548. 4. Sonnesen, Liselotte, and Peter Svensson. "Temporomandibular disor-ders and psychological status in adult patients with a deep bite." The European Journal of Orthodontics 30.6 (2008): 621-629. 5. Nicassio, Ralph, and Zavala, Maria. “Bone screw anchorage can reduce gingival display”. Journal of the American Orthodontic Society. January-February 2012:36-40. 6. Nicassio, Ralph, and Zavala, Maria. “TMJ Assessment and treatment Part 1: The relationship of the TMJ, growth & development and occlusion”. Journal of the American Orthodontic Society. Summer 2017:14-20. 7. Bartlett, David, and Geeta, Sundaram. "An up to 3-year randomized clinical study comparing indirect and direct resin composites used to restore worn posterior teeth." International Journal of Prosthodontics 19.6 (2006). Fig. 22 Fig. 23 even if we could advance the upper arch with reverse headgear, it is contraindicated if it would risk excessively and unaesthetically proclining upper incisors. Upper incisors ideally should be pointing right behind the orbit (upper 1-SN=102°). (Fig. 19) ᕢ Use orthognathic surgery to either advance the maxilla and/or perhaps setback the mandible. Most 8. Chander, N. Gopi, and R. Venkat. "An appraisal on increasing the occlusal vertical dimension in full occlusal rehabilitation and its outcome." The Journal of Indian Prosthodontic Society 11.2 (2011): 77. 9. Bite Guides. www.orthoarch.com. Sales2@orthoarch.com, 1-800-423-3527. 10. Chen, Yunn-Jy, et al. "Magnetic resonance images of the temporo-mandibular joints of patients with acquired open bite." Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 99.6 (2005): 734-742. 11. Nicassio, Ralph, and Zavala, Maria. “Variable Torque Brackets Enhance Treatment Outcomes”. Journal of the American Orthodontic Society. January-February 2013:34-40 22 Fall 2017 JAOS
Journal of the American Orthodontic Society Fall 2017: Page 22