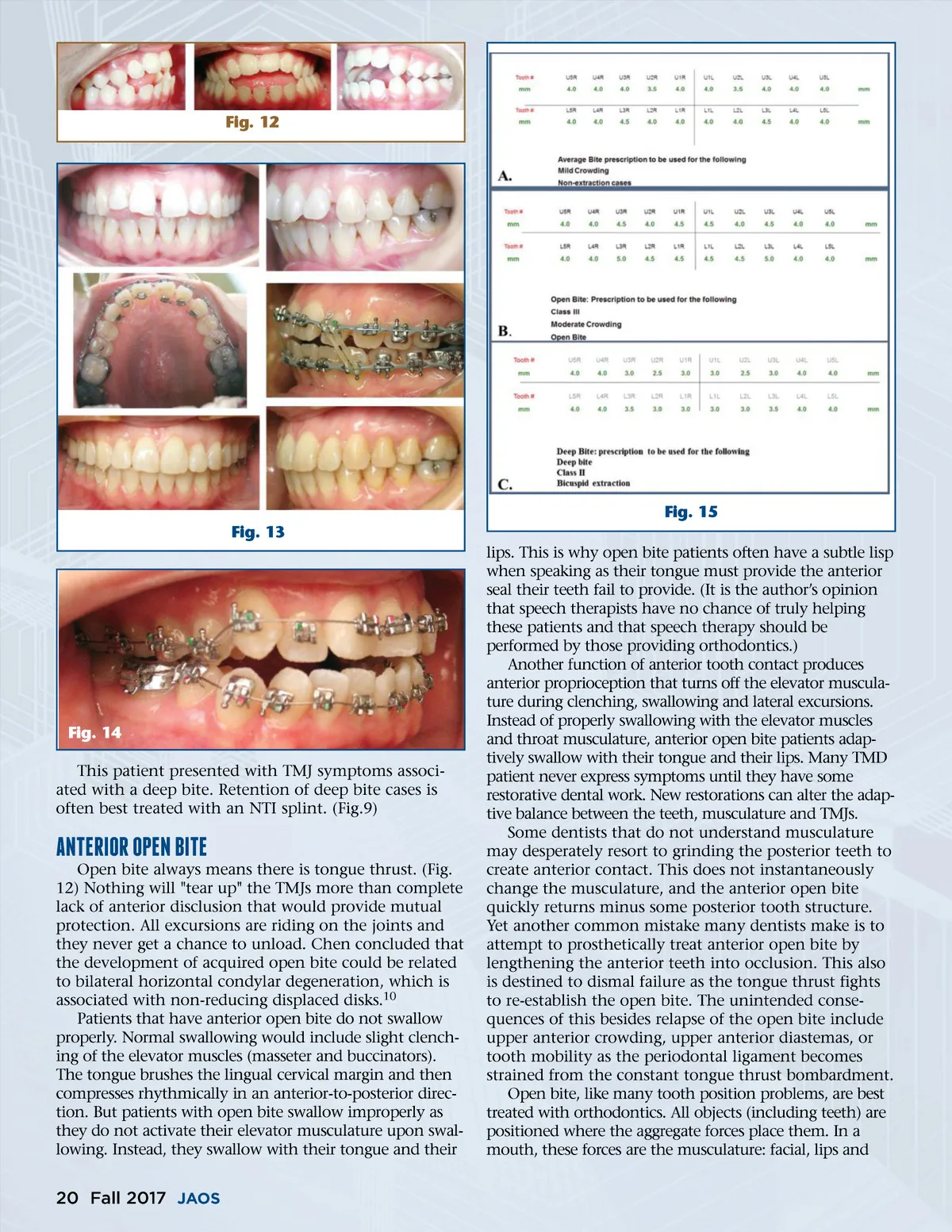
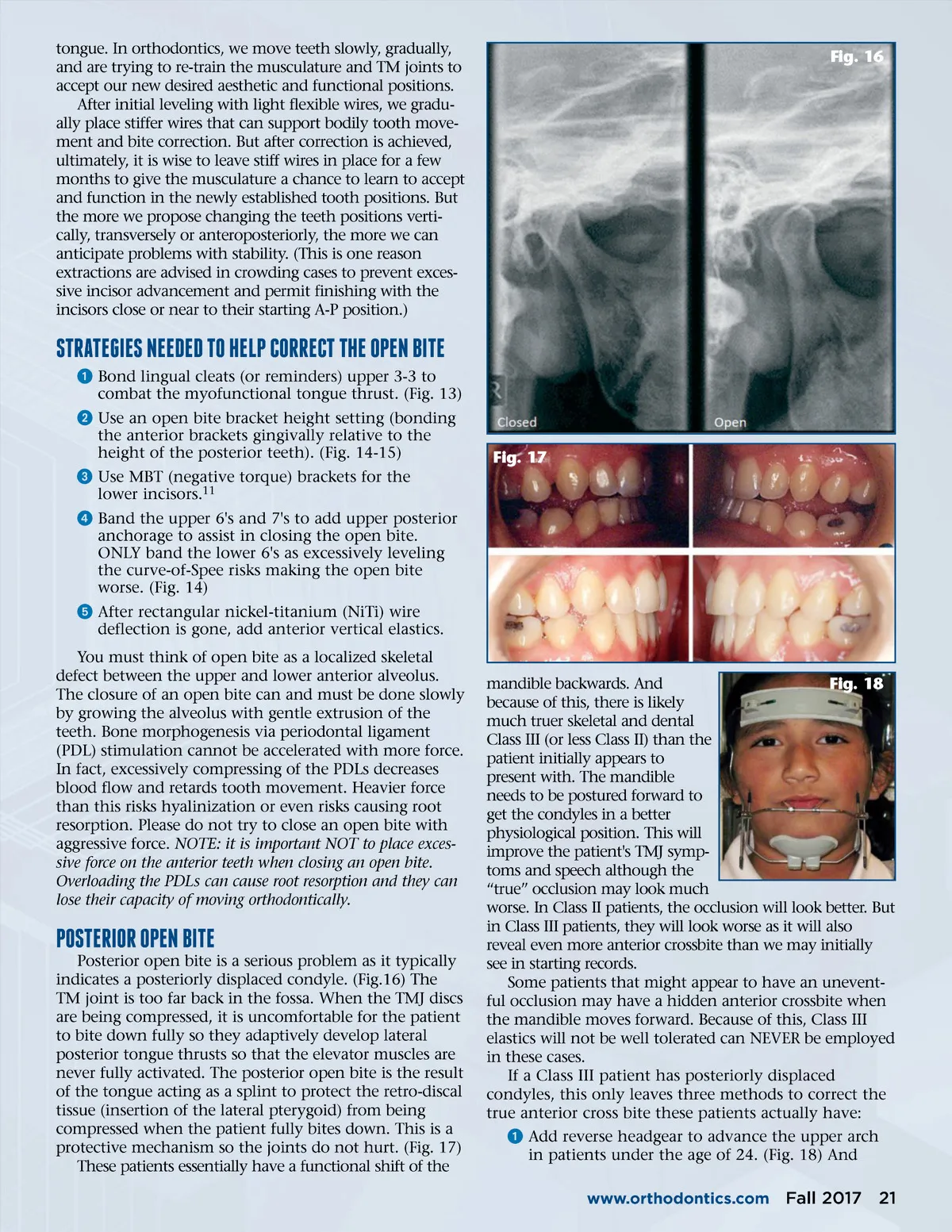
Fig. 12 Fig. 15 Fig. 13 lips. This is why open bite patients often have a subtle lisp when speaking as their tongue must provide the anterior seal their teeth fail to provide. (It is the author’s opinion that speech therapists have no chance of truly helping these patients and that speech therapy should be performed by those providing orthodontics.) Another function of anterior tooth contact produces anterior proprioception that turns off the elevator muscula-ture during clenching, swallowing and lateral excursions. Instead of properly swallowing with the elevator muscles and throat musculature, anterior open bite patients adap-tively swallow with their tongue and their lips. Many TMD patient never express symptoms until they have some restorative dental work. New restorations can alter the adap-tive balance between the teeth, musculature and TMJs. Some dentists that do not understand musculature may desperately resort to grinding the posterior teeth to create anterior contact. This does not instantaneously change the musculature, and the anterior open bite quickly returns minus some posterior tooth structure. Yet another common mistake many dentists make is to attempt to prosthetically treat anterior open bite by lengthening the anterior teeth into occlusion. This also is destined to dismal failure as the tongue thrust fights to re-establish the open bite. The unintended conse-quences of this besides relapse of the open bite include upper anterior crowding, upper anterior diastemas, or tooth mobility as the periodontal ligament becomes strained from the constant tongue thrust bombardment. Open bite, like many tooth position problems, are best treated with orthodontics. All objects (including teeth) are positioned where the aggregate forces place them. In a mouth, these forces are the musculature: facial, lips and Fig. 14 This patient presented with TMJ symptoms associ-ated with a deep bite. Retention of deep bite cases is often best treated with an NTI splint. (Fig.9) ANTERIOR OpEN BITE Open bite always means there is tongue thrust. (Fig. 12) Nothing will "tear up" the TMJs more than complete lack of anterior disclusion that would provide mutual protection. All excursions are riding on the joints and they never get a chance to unload. Chen concluded that the development of acquired open bite could be related to bilateral horizontal condylar degeneration, which is associated with non-reducing displaced disks. 10 Patients that have anterior open bite do not swallow properly. Normal swallowing would include slight clench-ing of the elevator muscles (masseter and buccinators). The tongue brushes the lingual cervical margin and then compresses rhythmically in an anterior-to-posterior direc-tion. But patients with open bite swallow improperly as they do not activate their elevator musculature upon swal-lowing. Instead, they swallow with their tongue and their 20 Fall 2017 JAOS
Journal of the American Orthodontic Society Fall 2017: Page 20