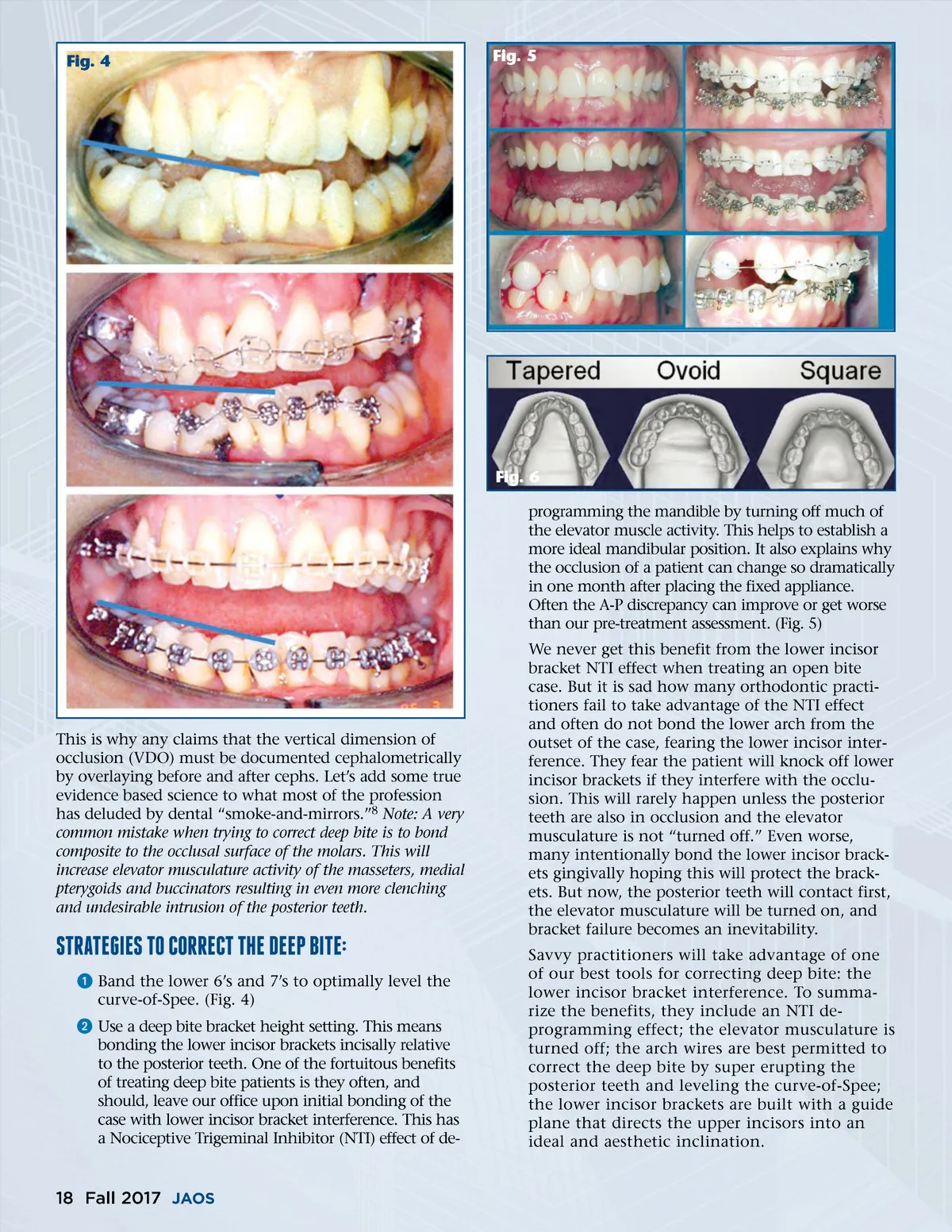
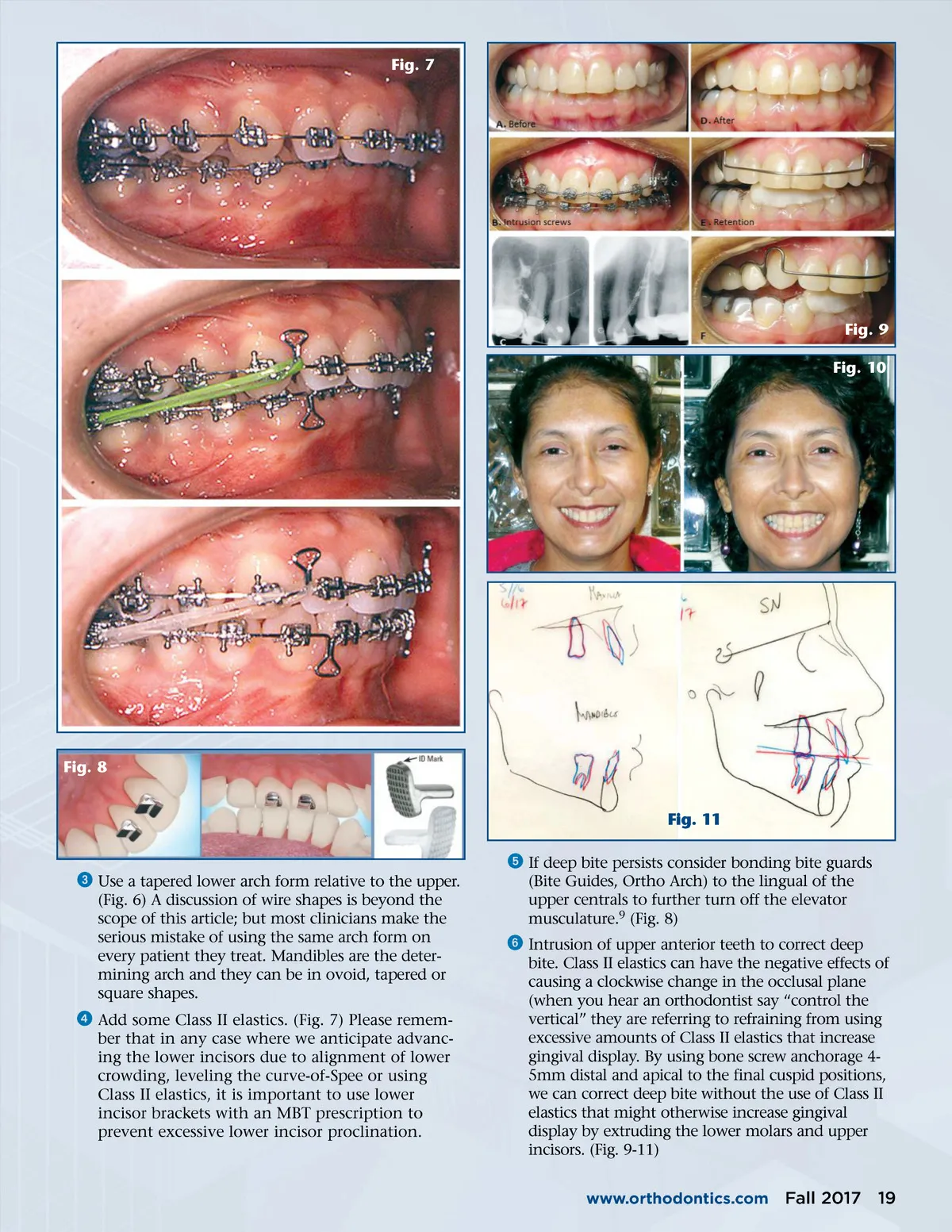
Fig. 4 Fig. 5 Fig. 6 programming the mandible by turning off much of the elevator muscle activity. This helps to establish a more ideal mandibular position. It also explains why the occlusion of a patient can change so dramatically in one month after placing the fixed appliance. Often the A-P discrepancy can improve or get worse than our pre-treatment assessment. (Fig. 5) We never get this benefit from the lower incisor bracket NTI effect when treating an open bite case. But it is sad how many orthodontic practi-tioners fail to take advantage of the NTI effect and often do not bond the lower arch from the outset of the case, fearing the lower incisor inter-ference. They fear the patient will knock off lower incisor brackets if they interfere with the occlu-sion. This will rarely happen unless the posterior teeth are also in occlusion and the elevator musculature is not “turned off.” Even worse, many intentionally bond the lower incisor brack-ets gingivally hoping this will protect the brack-ets. But now, the posterior teeth will contact first, the elevator musculature will be turned on, and bracket failure becomes an inevitability. Savvy practitioners will take advantage of one of our best tools for correcting deep bite: the lower incisor bracket interference. To summa-rize the benefits, they include an NTI de-programming effect; the elevator musculature is turned off; the arch wires are best permitted to correct the deep bite by super erupting the posterior teeth and leveling the curve-of-Spee; the lower incisor brackets are built with a guide plane that directs the upper incisors into an ideal and aesthetic inclination. This is why any claims that the vertical dimension of occlusion (VDO) must be documented cephalometrically by overlaying before and after cephs. Let’s add some true evidence based science to what most of the profession has deluded by dental “smoke-and-mirrors.” 8 Note: A very common mistake when trying to correct deep bite is to bond composite to the occlusal surface of the molars. This will increase elevator musculature activity of the masseters, medial pterygoids and buccinators resulting in even more clenching and undesirable intrusion of the posterior teeth. sTRATEgIEs TO CORRECT ThE DEEp BITE: ᕡ Band the lower 6’s and 7’s to optimally level the curve-of-Spee. (Fig. 4) ᕢ Use a deep bite bracket height setting. This means bonding the lower incisor brackets incisally relative to the posterior teeth. One of the fortuitous benefits of treating deep bite patients is they often, and should, leave our office upon initial bonding of the case with lower incisor bracket interference. This has a Nociceptive Trigeminal Inhibitor (NTI) effect of de-18 Fall 2017 JAOS
Journal of the American Orthodontic Society Fall 2017: Page 18